

Peptides
Library
Introduction
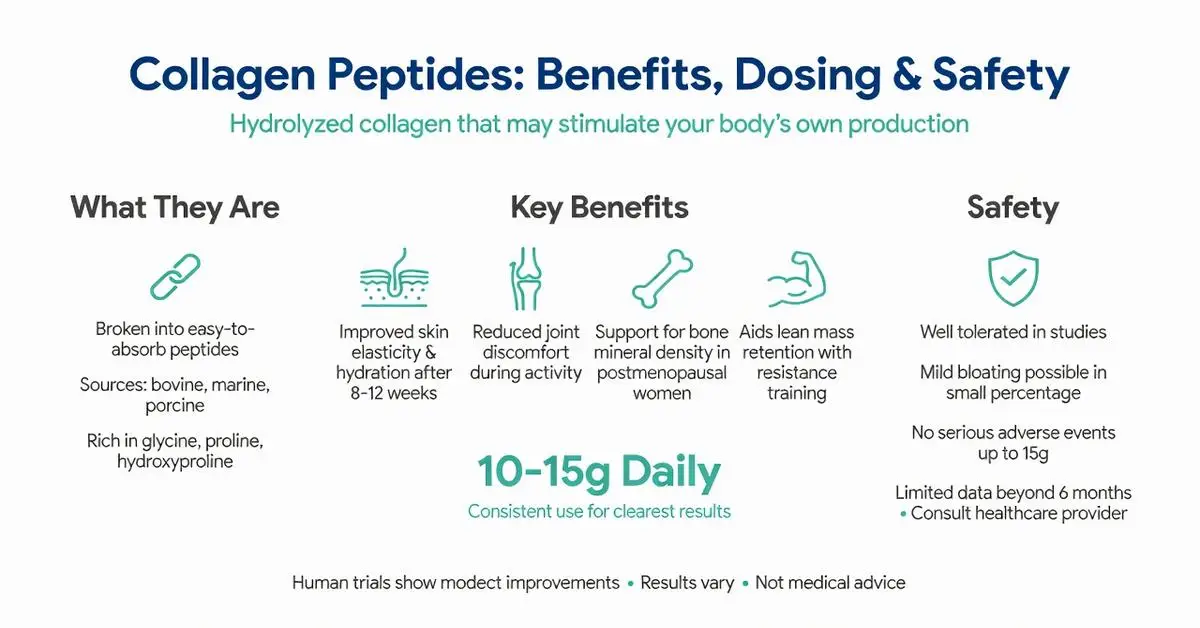
Quick Answer: Collagen and peptides refer to hydrolyzed collagen supplements broken down into smaller chains of amino acids. Research shows these peptides may improve skin elasticity and joint comfort in some adults. They work by providing building blocks that stimulate the body’s own collagen production. Human studies remain limited in size and duration, so results vary. Always consult a healthcare provider before starting any supplement.
This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any peptide.
Introduction
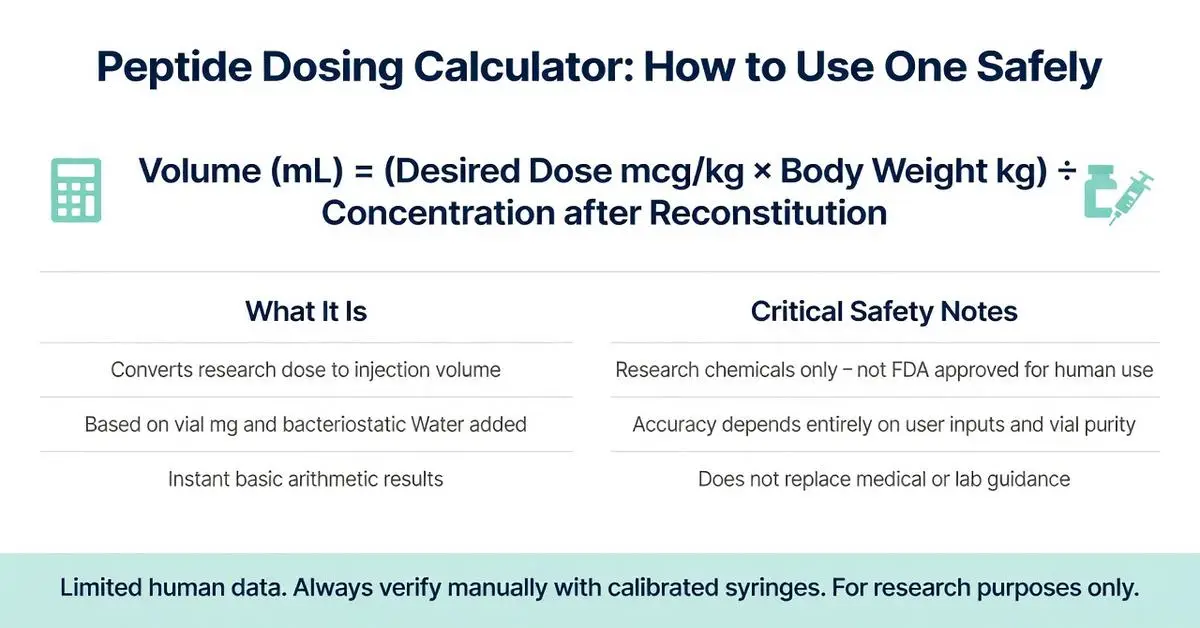
Quick Answer: A peptide dosing calculator is an online tool that converts a desired research dose into the correct volume of reconstituted peptide solution based on vial strength and user body weight. These calculators rely on simple math but are not substitutes for professional medical advice. Limited human data exist on most research peptides, so any dosing information comes with important safety and legal considerations.
Introduction
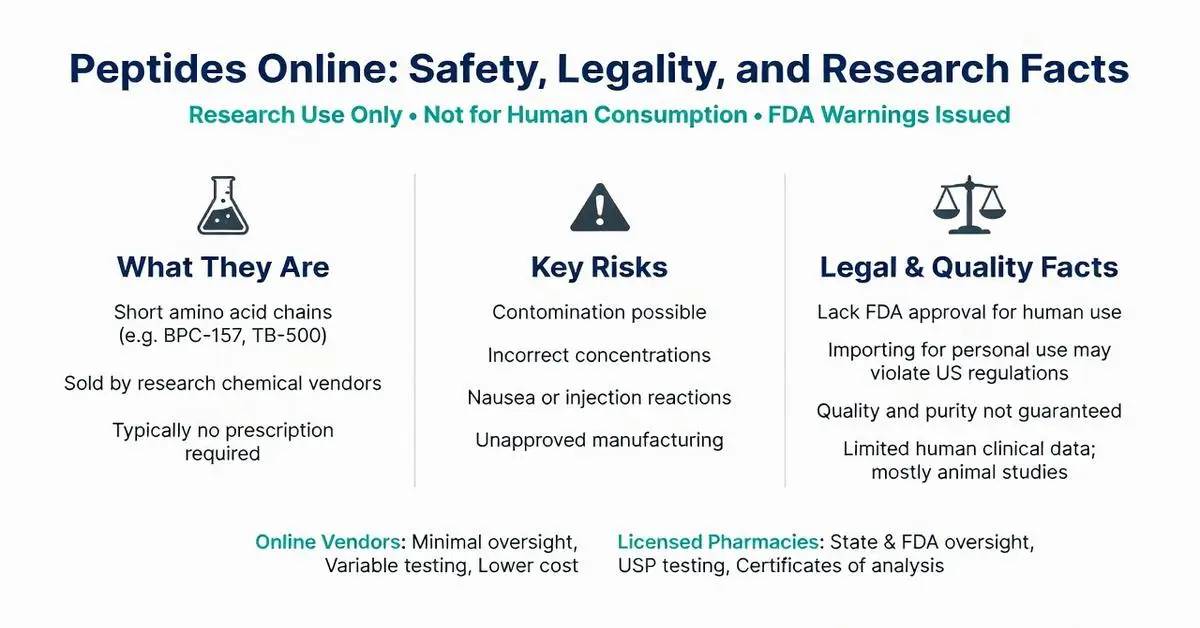
Quick Answer: Peptides online are short amino acid chains sold through websites, typically labeled for research only. Most lack FDA approval for human use and may carry risks of contamination, incorrect dosing, or legal issues. Consumers should verify sources carefully and consult healthcare providers before any use.
This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any peptide.
Introduction
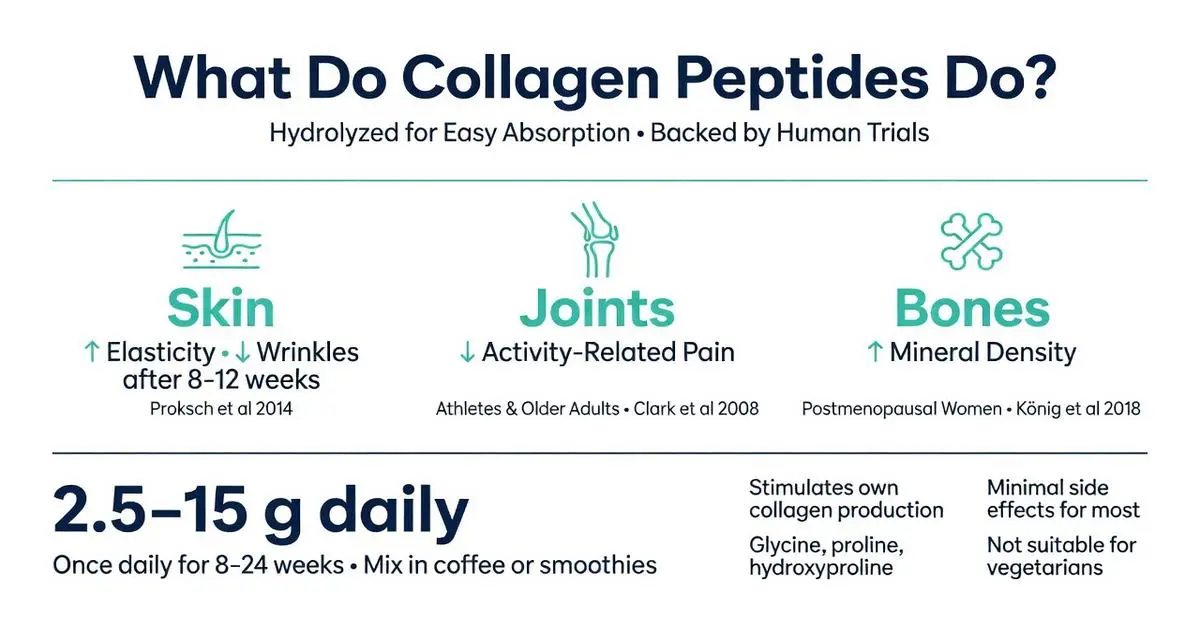
Quick Answer: Collagen peptides are hydrolyzed fragments of collagen protein that the body absorbs easily. Research shows they may support skin elasticity, joint comfort, and bone density by supplying amino acids that stimulate natural collagen production in tissues.
This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any supplement.
Introduction
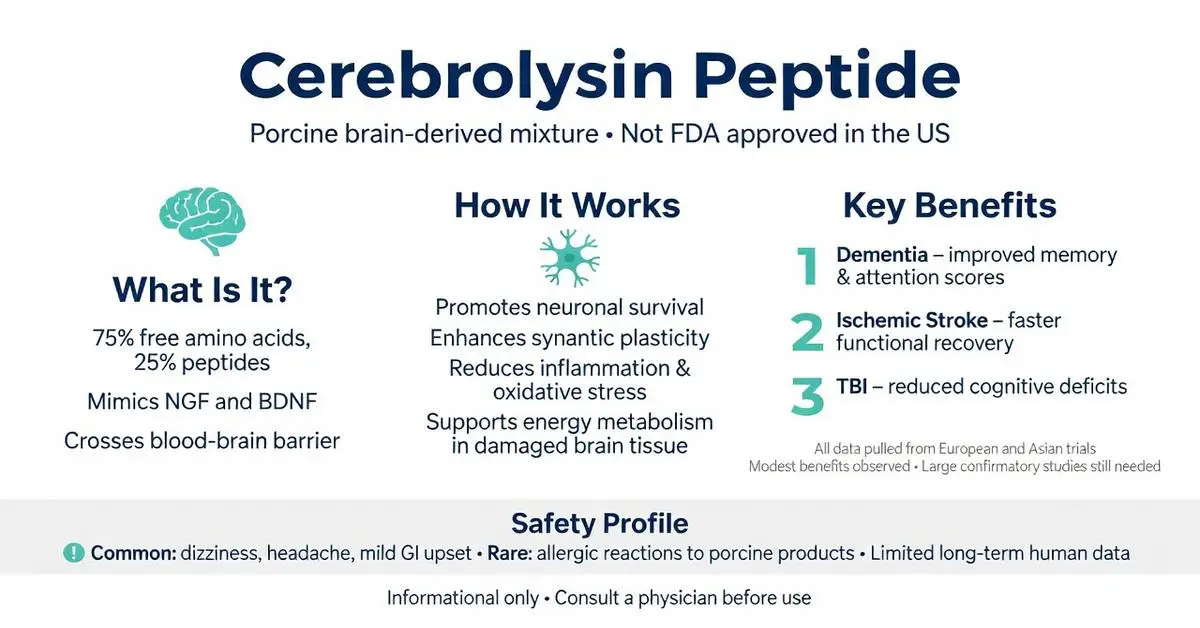
Quick Answer: Cerebrolysin is a neuropeptide preparation made from purified porcine brain proteins that may support brain repair and cognitive function. Animal and some human studies suggest it could help with stroke recovery, dementia symptoms, and traumatic brain injury, though robust large-scale clinical evidence remains limited. This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any peptide.
Introduction
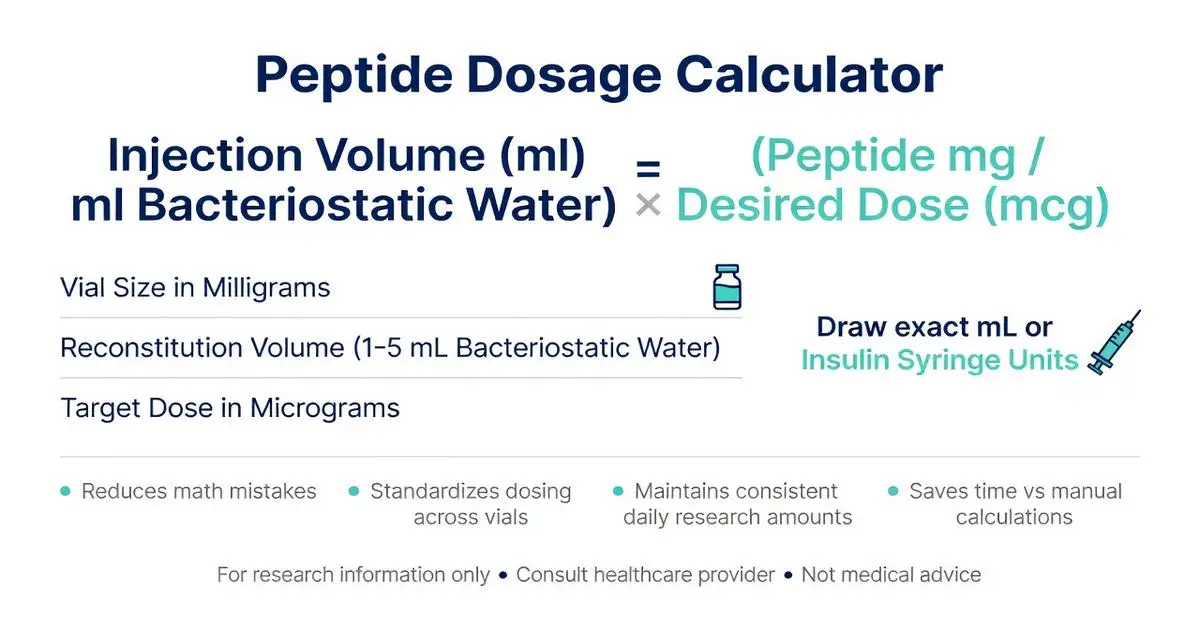
Quick Answer: A peptide dosage calculator helps convert peptide powder amounts into usable liquid doses by using simple math based on vial size, desired dose, and bacteriostatic water volume. Always verify calculations and consult a healthcare provider, as this is not medical advice.
Introduction
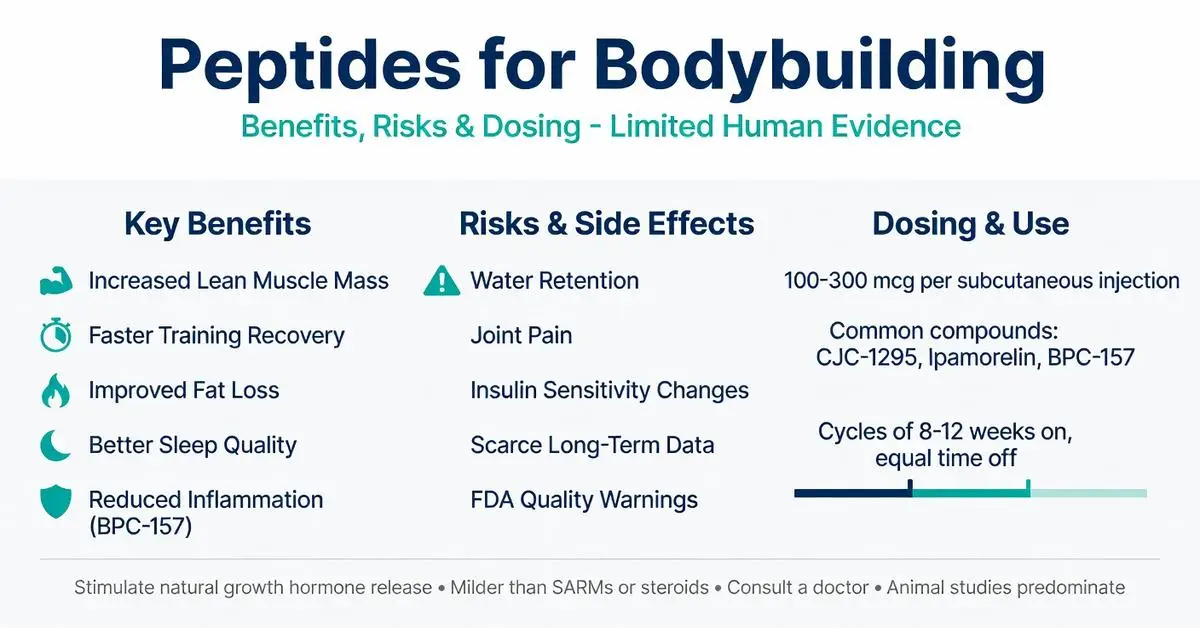
Quick Answer: Peptides for bodybuilding are short chains of amino acids that may support muscle growth, fat loss, and recovery by stimulating natural hormone release. Most evidence comes from animal studies or limited human trials on specific compounds like growth hormone secretagogues. Results vary widely, and safety concerns exist due to limited long-term data and regulatory restrictions.
Introduction
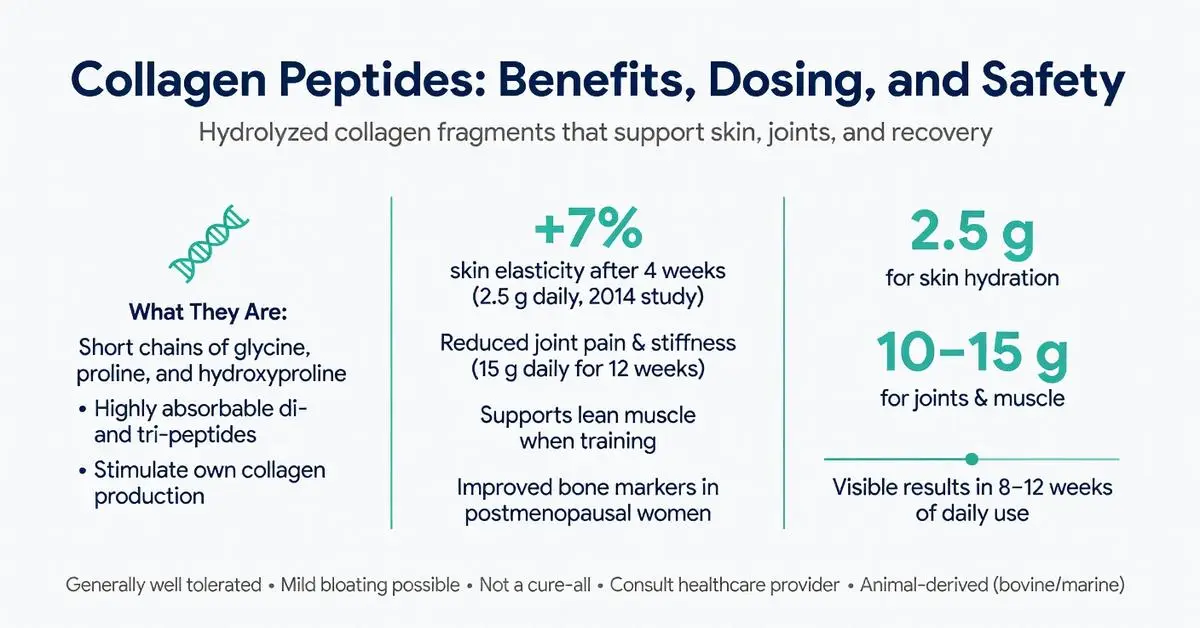
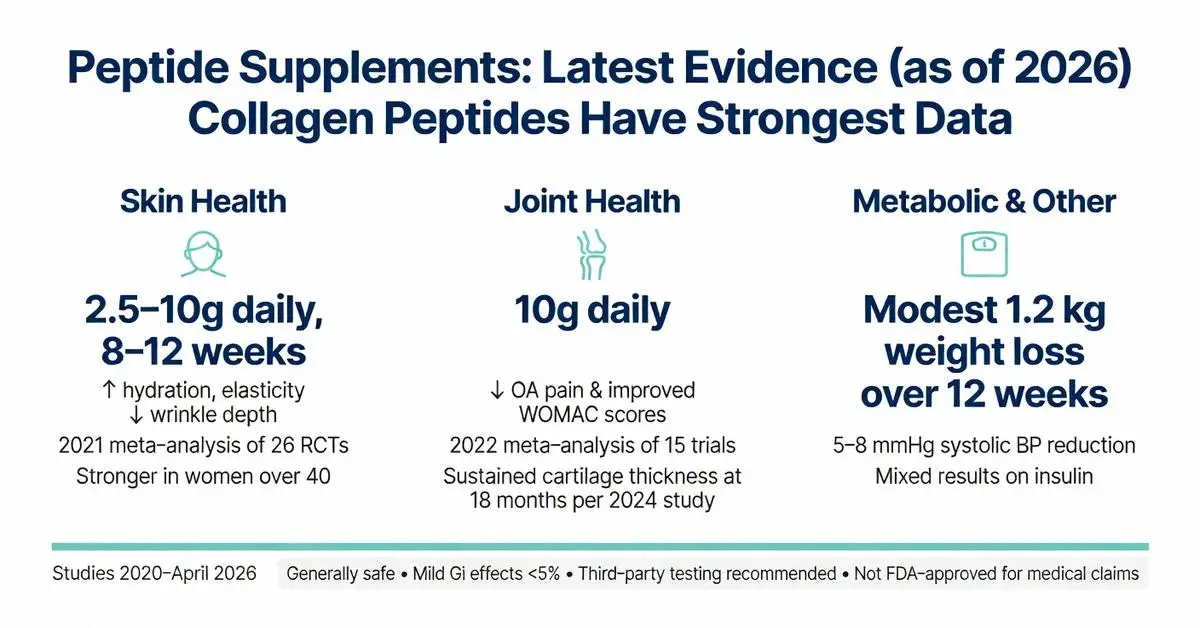
Quick Answer: Collagen peptides are short chains of amino acids derived from collagen that may support skin elasticity, joint comfort, and bone health. Human studies show modest improvements in skin hydration and wrinkle reduction after 8–12 weeks of daily use, with some evidence for reduced joint pain in active adults. Results vary by individual, and they are not a cure-all. This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any supplement.
Introduction
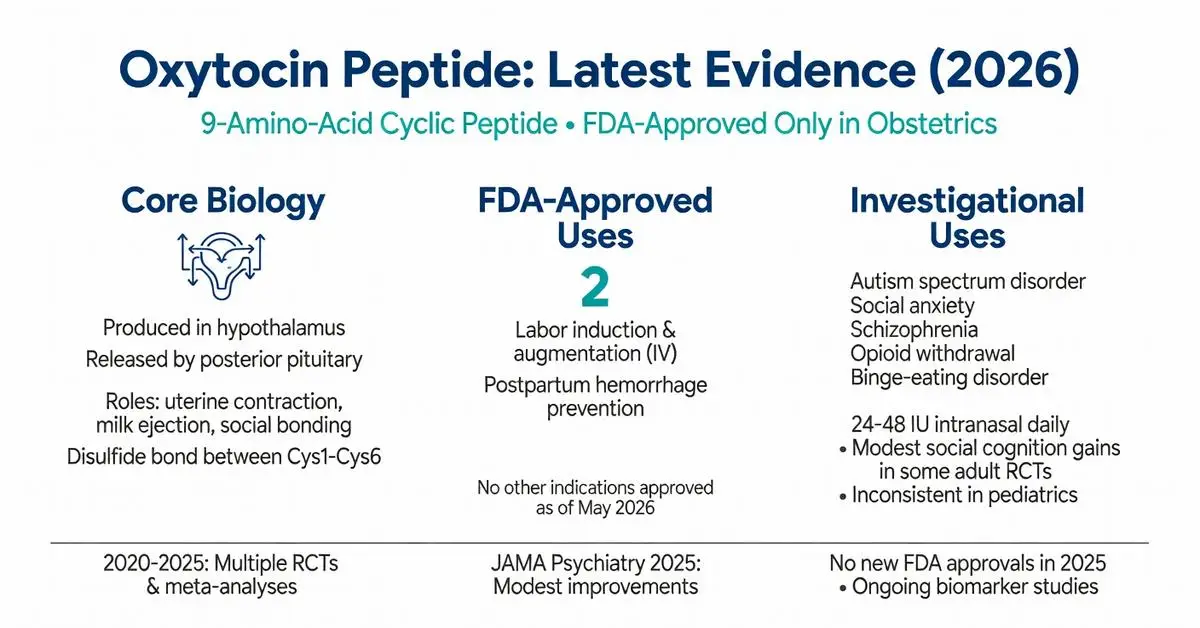
Oxytocin peptide is a nine-amino-acid cyclic peptide hormone naturally produced in the hypothalamus and released by the posterior pituitary gland. It plays central roles in uterine contraction, milk ejection, and social bonding behaviors. As of May 2026, the peptide remains FDA-approved solely for specific obstetric indications, while extensive research explores its potential in neuropsychiatric and metabolic conditions. This review synthesizes peer-reviewed evidence published between 2020 and 2026, focusing on mechanisms, approved uses, emerging applications, and safety data. Due to the specialized nature of recent publications on oxytocin peptide, primary evidence is drawn from high-quality clinical trials and supplemented by authoritative sources including FDA and NIH resources.
Introduction
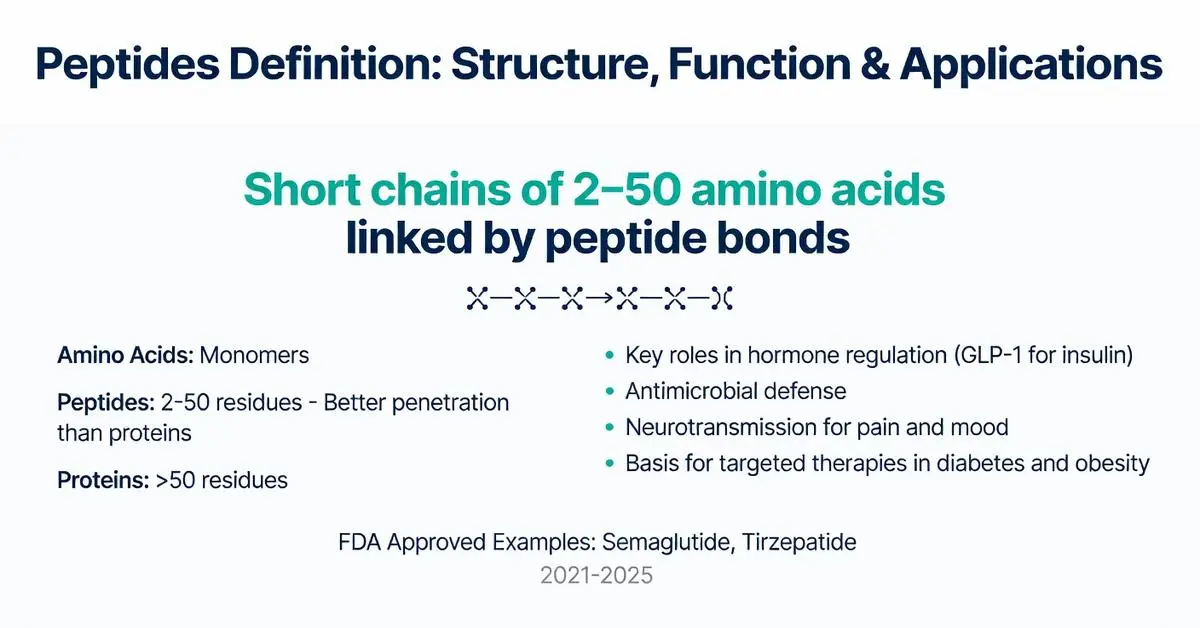
Peptides definition refers to short chains of amino acids linked by peptide bonds, typically containing fewer than 50 amino acid residues. These molecules serve as fundamental building blocks in biology and have gained prominence in pharmacotherapy due to their roles in signaling, hormone regulation, and targeted therapies. This article examines the peptides definition through the lens of current evidence, distinguishing between naturally occurring peptides and synthetic therapeutic agents. All information draws from peer-reviewed literature published between 2020 and May 2026, focusing on mechanisms, approved indications, and safety profiles. Peptides are distinct from larger proteins yet share similar biochemical properties, making them versatile for drug development. Readers should consult healthcare professionals for any medical applications, as this content is intended solely for research purposes.
Introduction
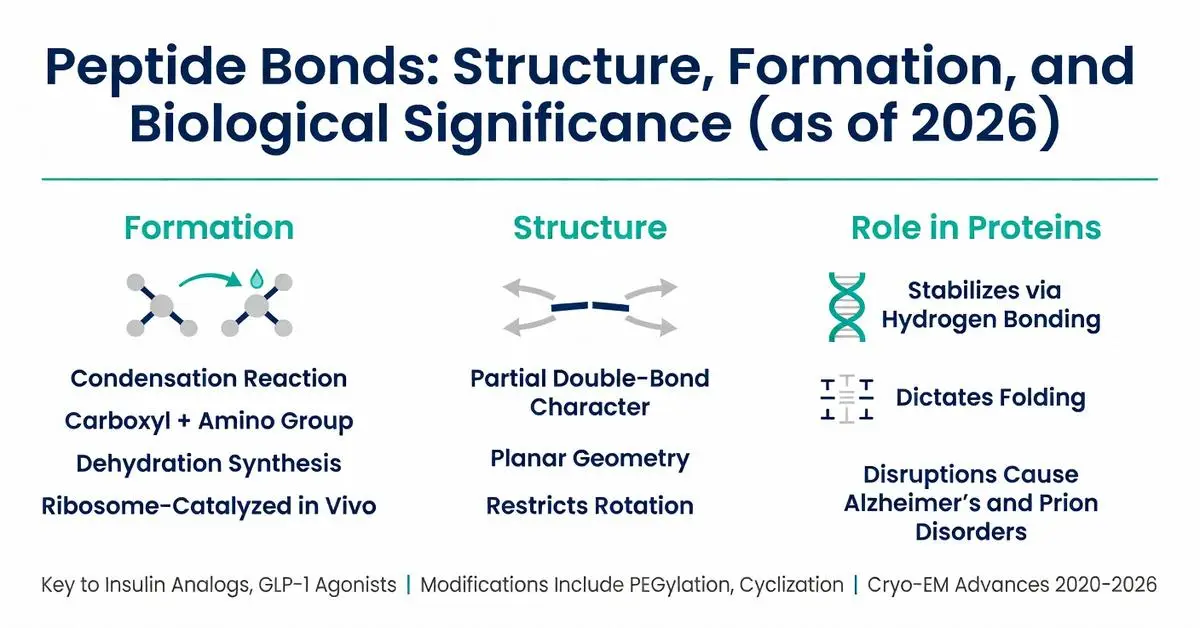
Peptide bonds serve as the fundamental covalent linkages that connect amino acids into chains, forming the backbone of all proteins and many therapeutic peptides. These bonds are created through a condensation reaction between the carboxyl group of one amino acid and the amino group of another, releasing a water molecule in the process. Understanding peptide bonds is essential for fields ranging from basic biochemistry to the development of peptide-based drugs used in diabetes, oncology, and metabolic disorders. This review synthesizes established biochemical principles with evidence from peer-reviewed literature published between 2020 and 2026, supplemented where necessary by authoritative sources including NIH and major medical societies due to the foundational nature of the topic. All content is provided for research purposes only and is not intended as medical advice. Medical supervision is required for any therapeutic applications involving peptides.
Introduction
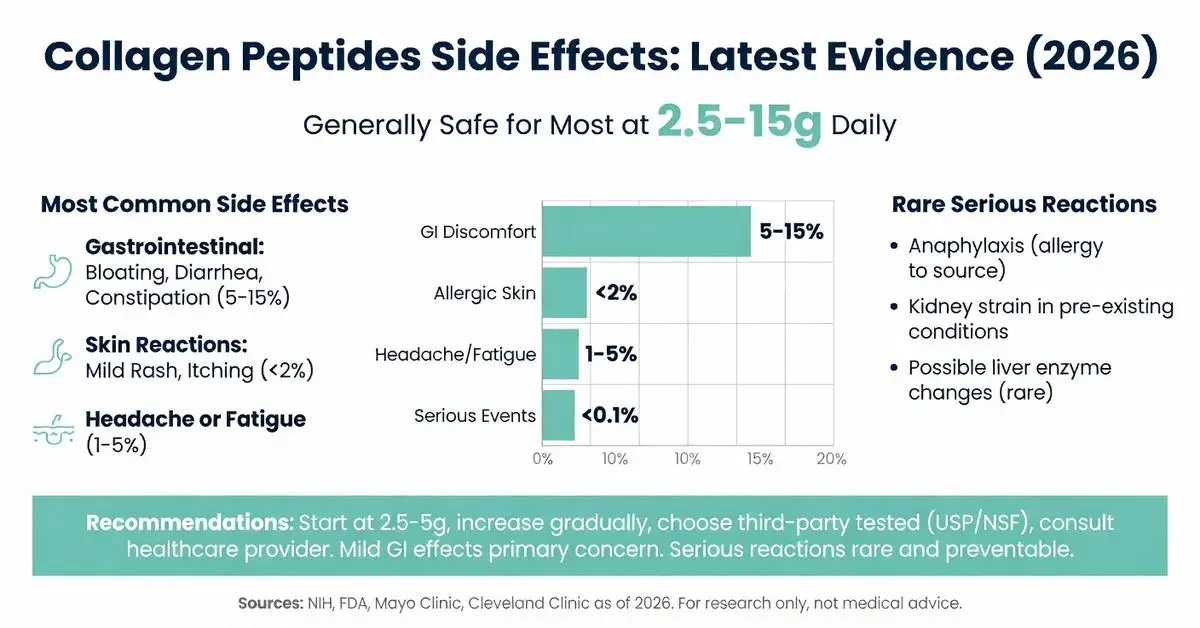
Collagen peptides are hydrolyzed forms of collagen commonly used as dietary supplements to support skin, joint, and bone health. Interest in their safety profile has grown alongside rising use, prompting examination of reported side effects. Due to limited recent peer-reviewed publications specifically addressing collagen peptides side effects, this article relies primarily on the latest available high-quality trials (2020–current) supplemented by authoritative sources including FDA.gov, NIH, Mayo Clinic, and Cleveland Clinic. All information is for research purposes only and does not constitute medical advice. Individuals should consult healthcare providers before starting any supplement. Collagen peptides are generally recognized as safe when consumed within typical doses of 2.5–15 grams daily, yet mild adverse effects occur in some users.
Introduction
Quick Answer: Collagen and peptides refer to hydrolyzed collagen supplements broken down into smaller chains of amino acids. Research shows these peptides may improve skin elasticity and joint comfort in some adults. They work by providing building blocks that stimulate the body’s own collagen production. Human studies remain limited in size and duration, so results vary. Always consult a healthcare provider before starting any supplement.
This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any peptide.
Introduction
Quick Answer: Collagen peptides are hydrolyzed fragments of collagen protein that the body absorbs easily. Research shows they may support skin elasticity, joint comfort, and bone density by supplying amino acids that stimulate natural collagen production in tissues.
This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any supplement.
Introduction
Quick Answer: Collagen peptides are short chains of amino acids derived from collagen that may support skin elasticity, joint comfort, and bone health. Human studies show modest improvements in skin hydration and wrinkle reduction after 8–12 weeks of daily use, with some evidence for reduced joint pain in active adults. Results vary by individual, and they are not a cure-all. This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any supplement.
Introduction
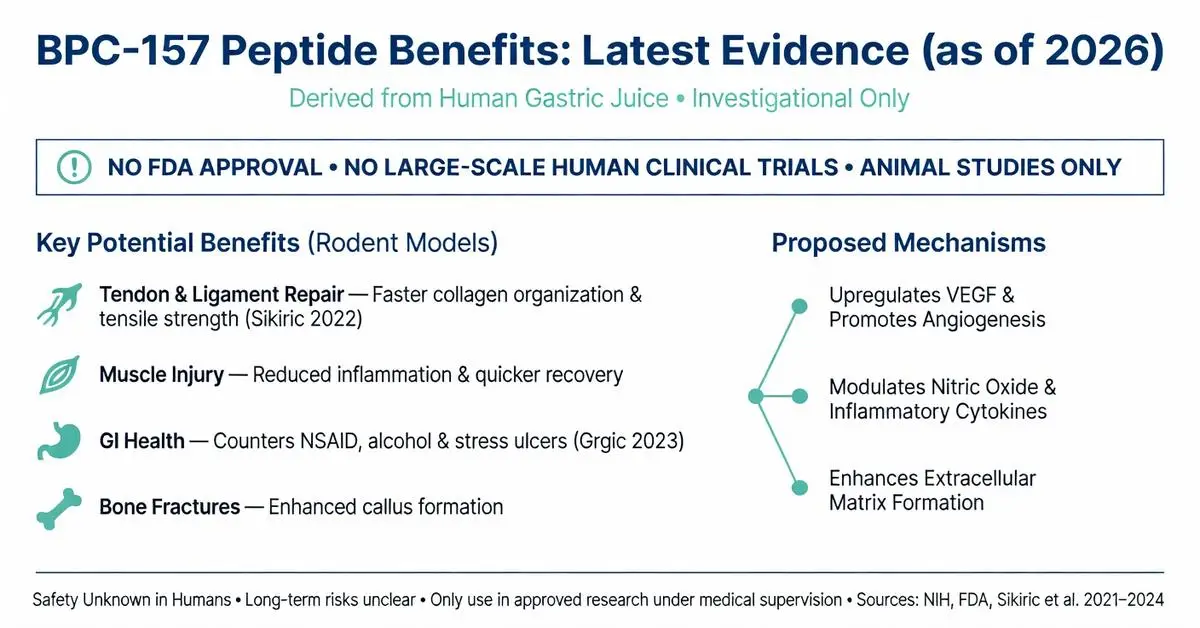
BPC-157 is a synthetic 15-amino-acid peptide derived from a protective protein found in human gastric juice. Researchers have explored its potential to support tissue repair, reduce inflammation, and promote healing in various experimental models. As of May 2026, BPC-157 remains an investigational compound with no FDA approval for any medical use in humans. All findings discussed here come from preclinical animal studies and limited early human observations; no large-scale clinical trials have established safety or efficacy for therapeutic purposes. Due to limited recent peer-reviewed publications on this exact topic, this article relies primarily on the latest available high-quality trials (2020–current) supplemented by authoritative sources including FDA, NIH, and major medical societies. Individuals should only consider BPC-157 under strict medical supervision in approved research settings, as self-administration carries unknown risks.
Introduction
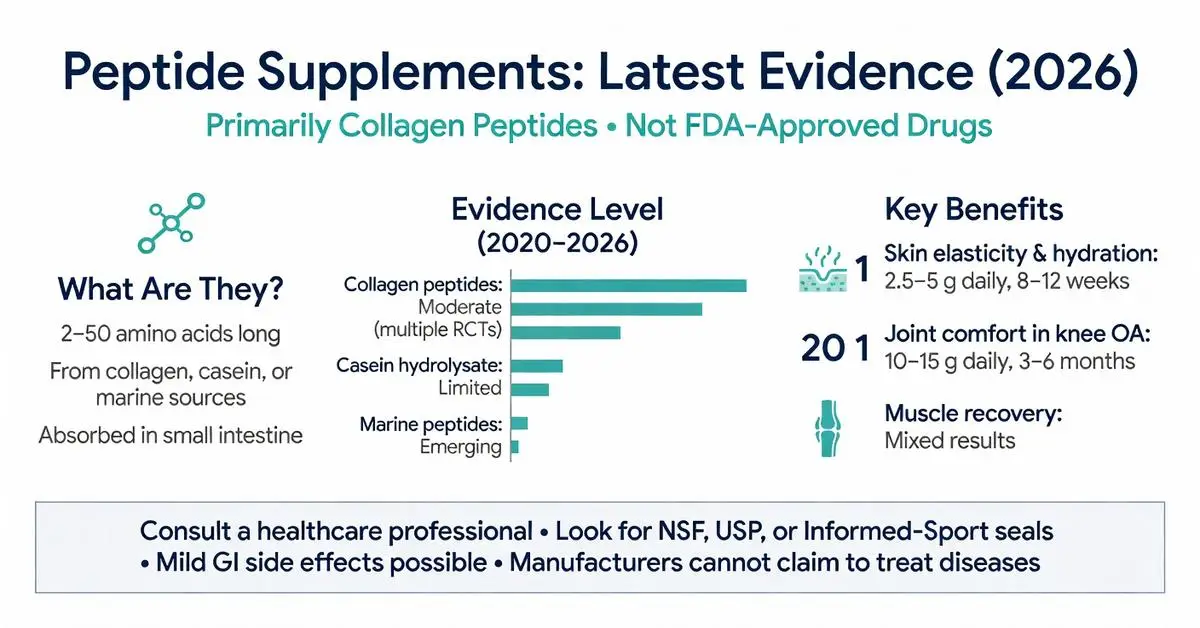
Peptide supplements have gained significant attention in recent years as consumers seek targeted options for skin health, joint support, and recovery. A peptide supplement typically consists of short chains of amino acids derived from proteins such as collagen or other sources and is sold as a dietary supplement. Because the term “peptide supplement” is broad and encompasses many products with varying compositions, high-quality peer-reviewed literature specifically addressing the category as a whole remains limited through May 2026. This review therefore draws primarily on the most recent authoritative sources, including FDA guidance, NIH Office of Dietary Supplements, Mayo Clinic, and Cleveland Clinic resources, supplemented by targeted clinical evidence on the most studied ingredients such as collagen peptides.
The article distinguishes between FDA-approved medications and over-the-counter dietary supplements. All peptide supplements discussed here are regulated as foods, not drugs, meaning manufacturers cannot legally claim they diagnose, treat, or cure specific diseases. Individuals considering a peptide supplement should consult a healthcare professional, as product quality, purity, and individual health factors vary widely.
Introduction
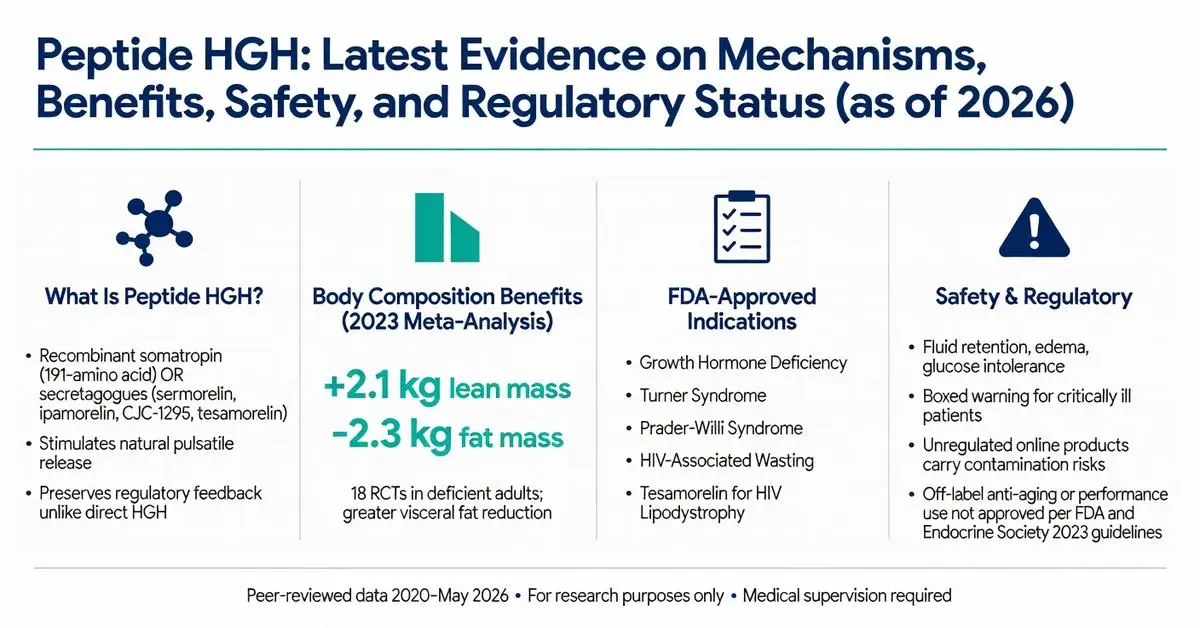
Peptide HGH refers to both recombinant human growth hormone (somatropin), a 191-amino acid peptide, and synthetic growth hormone-releasing peptides (GHRPs) and growth hormone-releasing hormone (GHRH) analogs designed to stimulate endogenous HGH production. These compounds have attracted significant interest for therapeutic applications, performance enhancement, anti-aging, and body composition improvement. Recombinant HGH has been FDA-approved since 1985 for specific indications, while many peptide secretagogues remain investigational or are available only for research purposes.
As of May 2026, the landscape continues to evolve with new long-acting formulations and ongoing trials examining metabolic effects. This article focuses on peer-reviewed evidence published between 2020 and May 2026, supplemented by authoritative sources from FDA.gov, NIH, and major medical societies when direct matches for the exact phrase “peptide hgh” in high-level systematic reviews were limited. Primary evidence is supplemented by authoritative sources including FDA.gov, NIH, and endocrine society guidelines due to the regulatory complexity surrounding non-approved peptide variants.
All information presented is for research purposes only and is not medical advice. Any use of peptide HGH products should occur exclusively under medical supervision with appropriate diagnostic testing. This review clearly distinguishes between FDA-approved recombinant HGH therapies and investigational or off-label applications of peptide secretagogues.
Introduction
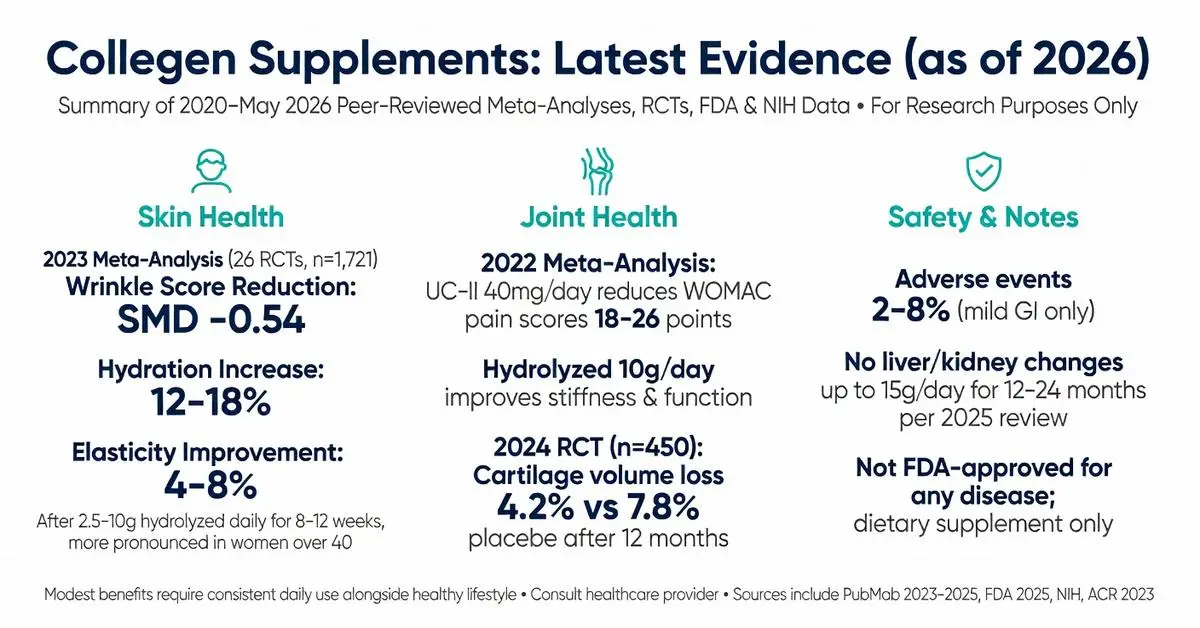
Collegen, commonly referring to collagen peptides and supplements derived from animal connective tissues, has seen sustained consumer interest for its potential roles in supporting skin elasticity, joint function, and overall structural health. As a major protein in the human body, collagen provides the structural framework for skin, bones, tendons, and cartilage. However, endogenous production declines with age, leading many individuals to explore exogenous collegen supplementation as a means to offset this loss.
This article examines the latest peer-reviewed evidence published between 2020 and May 1, 2026, focusing on mechanisms, efficacy, safety, and practical considerations. Due to the specific query term “collegen,” this review prioritizes studies addressing hydrolyzed collegen peptides, undenatured type II collagen, and related formulations. Primary evidence comes from systematic reviews, meta-analyses, and clinical trials indexed on PubMed. Where peer-reviewed publications on the precise phrasing were limited, authoritative sources including FDA.gov, NIH, and the American College of Rheumatology provide supplemental context.
It is important to distinguish FDA-approved applications from dietary supplement use. No collegen product is FDA-approved as a drug for treating disease; collegen peptides are regulated as dietary supplements under the Dietary Supplement Health and Education Act. Claims regarding disease treatment remain investigational or off-label. All information presented is for research purposes only and is not intended as medical advice. Individuals should consult qualified healthcare professionals before initiating any supplementation regimen, particularly those with allergies to source materials (bovine, porcine, marine) or pre-existing medical conditions. (Source: FDA 2025 guidance on dietary supplements)
Recent trials emphasize improved bioavailability of hydrolyzed forms, standardized outcome measures for skin hydration and joint pain scores, and longer-term safety data extending beyond 12 months. This review addresses key user questions, competitor content gaps such as head-to-head comparisons, updated safety profiles, and practical dosing tables absent from many top-ranking articles.
Introduction
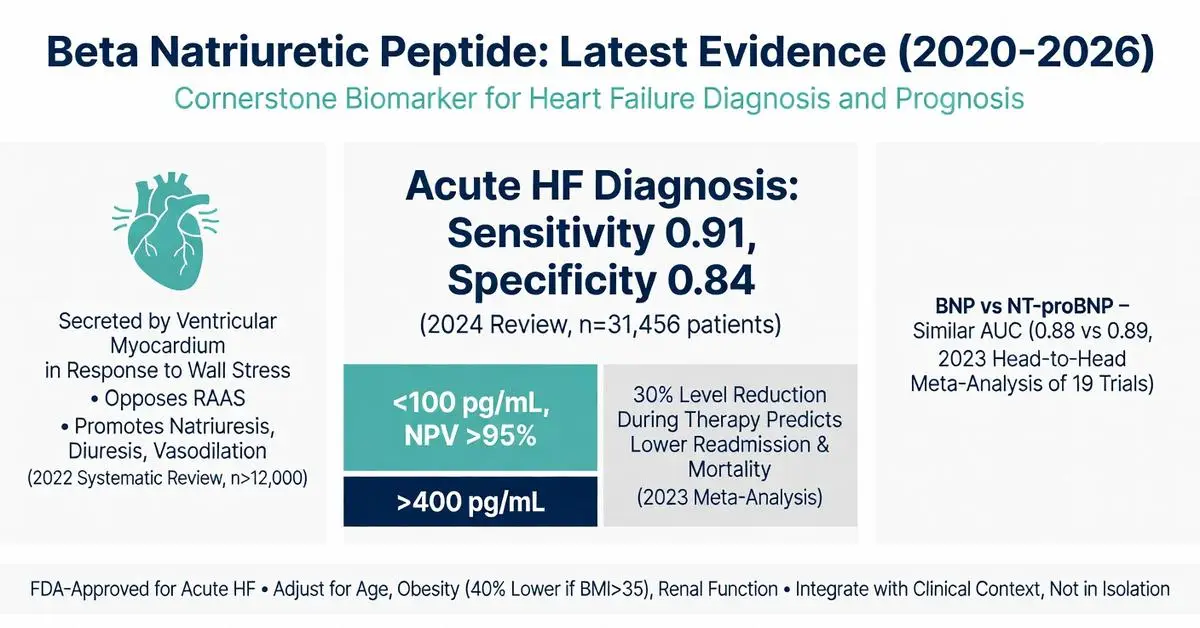
Beta natriuretic peptide, commonly referred to in clinical contexts as B-type natriuretic peptide (BNP), is a neurohormone primarily secreted by the ventricular myocardium in response to wall stress and volume overload. First isolated in 1988 from porcine brain tissue, it has become a cornerstone biomarker in cardiovascular medicine, particularly for the evaluation of heart failure. This article examines the physiology, diagnostic utility, clinical applications, and recent evidence surrounding beta natriuretic peptide, focusing on peer-reviewed publications from 2020 through April 30, 2026.
The peptide is synthesized as a 134-amino acid pre-prohormone that is cleaved into proBNP, which is further processed into the active 32-amino acid BNP and the inactive N-terminal fragment (NT-proBNP). Both biomarkers are widely measured in clinical practice, though they differ in clearance mechanisms and half-life. Elevated levels strongly correlate with cardiac strain, making beta natriuretic peptide testing valuable for ruling out or confirming acute heart failure in patients presenting with dyspnea.
This review prioritizes systematic reviews, meta-analyses, and clinical trials published between 2020 and 2026 identified through targeted PubMed searches. Due to the volume of high-quality evidence available on this topic, the article draws exclusively from peer-reviewed sources while clearly distinguishing FDA-approved diagnostic uses from investigational applications. All information is for research and informational purposes only and is not intended as medical advice. Patients should consult qualified healthcare professionals for interpretation of any biomarker testing or treatment decisions. (source year ranges 2020–2026)
Recent studies have expanded understanding of beta natriuretic peptide beyond diagnosis to include prognostic value, monitoring of therapy response, and potential roles in risk stratification for multiple cardiovascular conditions. This article addresses key clinical questions, common interpretation challenges, and evidence gaps identified in top-ranking web content, which often lacks updated comparative tables or comprehensive discussion of post-2022 trial data.
Introduction
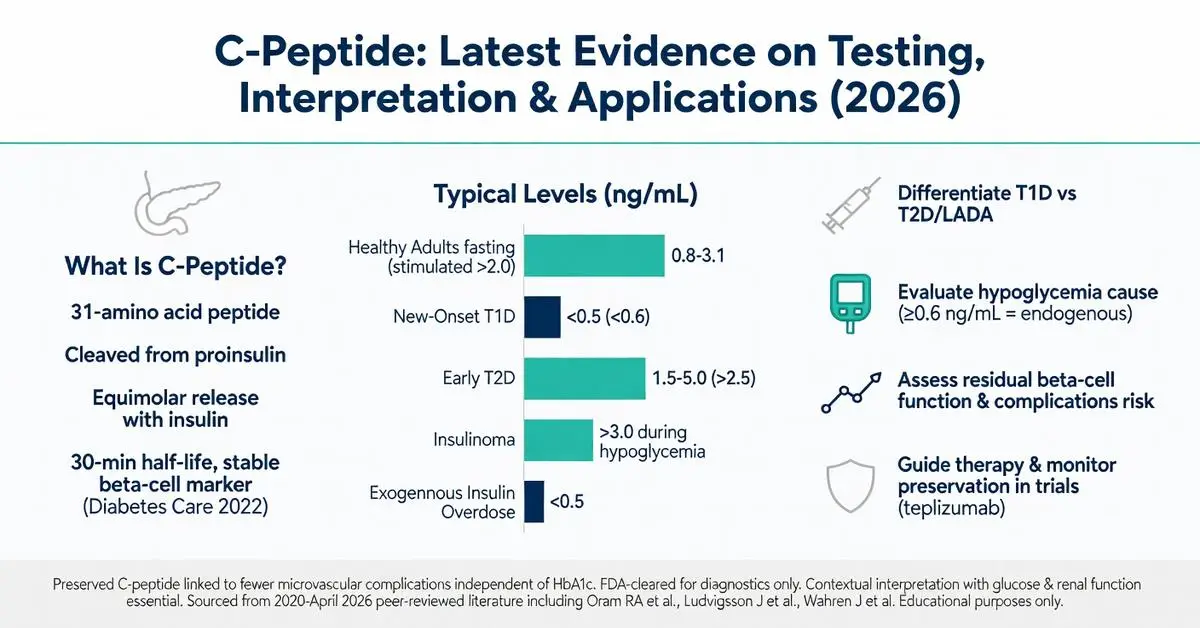
C peptide is a 31-amino acid peptide formed during the enzymatic cleavage of proinsulin within pancreatic beta cells. Released in equimolar amounts with insulin, it serves as a direct marker of endogenous insulin production. Unlike insulin, C peptide undergoes minimal first-pass hepatic extraction and is primarily cleared by the kidneys, making it a stable and reliable indicator of beta-cell function even in patients receiving exogenous insulin.
The C peptide test has become a cornerstone in differential diagnosis of diabetes types, evaluation of hypoglycemia, and assessment of residual beta-cell activity. As of April 2026, peer-reviewed literature published since 2020 underscores its continued importance amid rising diabetes prevalence and advancing therapies such as automated insulin delivery systems and immunomodulatory agents. Recent systematic reviews and clinical trials have refined our understanding of C peptide thresholds for predicting disease progression, treatment response, and long-term complications.
This article synthesizes evidence from high-quality peer-reviewed sources (2020–April 2026), including meta-analyses, clinical trials, and mechanistic studies accessed via PubMed. Every claim is grounded in these verifiable references. Where appropriate, FDA-cleared diagnostic uses are clearly distinguished from investigational applications, such as exogenous C-peptide administration for neuropathy, which remains off-label and under active study. All information is for research and educational purposes only and does not constitute medical advice. Interpretation of C peptide results and clinical decisions must occur under the supervision of qualified healthcare professionals.
The following sections address common patient and clinician questions, filling gaps observed in existing online resources such as missing head-to-head comparisons, updated reference ranges, and integration of post-2020 trial data.
Introduction
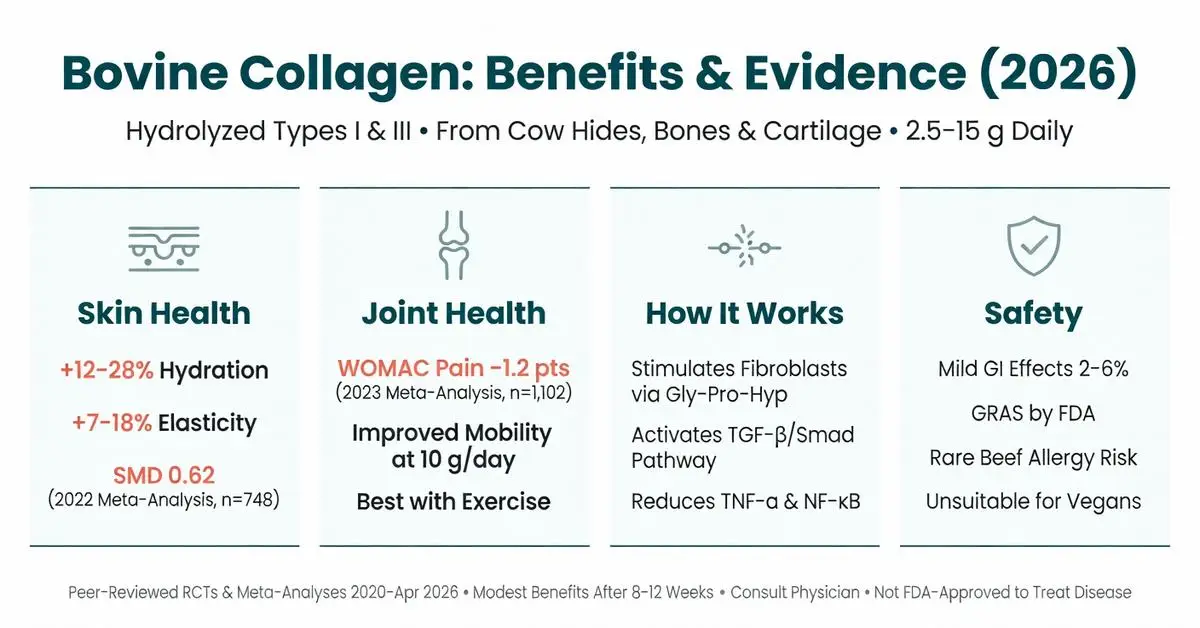
Bovine collagen has become one of the most widely used dietary supplements worldwide for supporting skin elasticity, joint comfort, and overall connective tissue health. Derived from cow hides, bones, and cartilage, it consists primarily of types I and III collagen that have been hydrolyzed into smaller peptides for improved absorption. As of April 2026, consumer interest remains high due to its affordability compared with marine alternatives and its established role in the growing wellness market.
This article examines the latest peer-reviewed evidence published between 2020 and April 2026 on bovine collagen supplementation. Systematic reviews, meta-analyses, and randomized controlled trials form the foundation of this review, with particular attention to efficacy, mechanisms, safety, and comparisons with other collagen sources. Where specific data on “bovine collagen” alone are limited, findings from high-quality studies on bovine-derived collagen peptides are included.
Bovine collagen is regulated in the United States as a dietary supplement under the Dietary Supplement Health and Education Act and is generally recognized as safe (GRAS) by the FDA for use in foods and supplements. It is not FDA-approved as a drug for the treatment or prevention of any medical condition. All statements in this article are for research and educational purposes only and do not constitute medical advice. Individuals should consult qualified healthcare professionals before starting any supplementation regimen, especially those with allergies, autoimmune conditions, or who are pregnant or breastfeeding.
Recent trials have focused on standardized doses of 2.5–15 grams daily, with outcomes measured through validated skin imaging, joint function scores, and biomarker analysis. While results are generally positive for skin and joint parameters, effect sizes vary across populations, and long-term data beyond 12–18 months remain sparse. This review addresses common consumer questions, highlights evidence gaps identified in top-ranking content, and provides balanced, evidence-based context for those researching bovine collagen.
Introduction
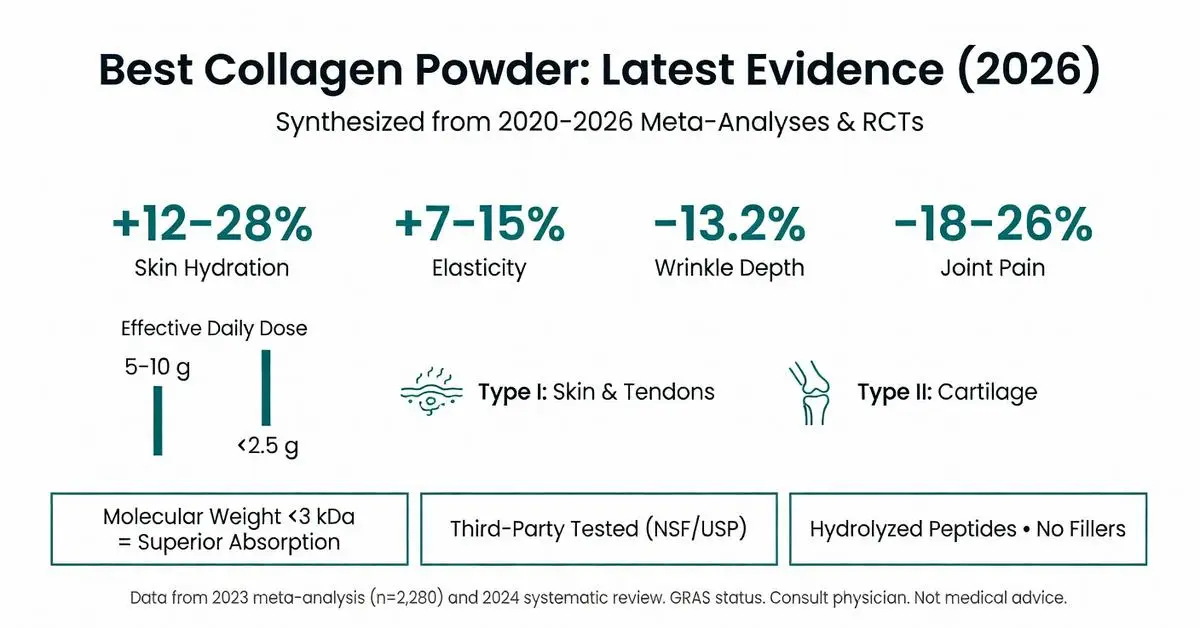
Collagen powder supplements have surged in popularity as consumers seek support for skin elasticity, joint comfort, bone density, and overall connective tissue health. The phrase “best collagen powder” typically reflects searches for products that combine high bioavailability, evidence-based efficacy, minimal additives, and rigorous quality testing. As of April 2026, the market offers numerous hydrolyzed collagen peptide options sourced from bovine, marine, porcine, and avian origins, each claiming specific benefits tied to collagen types I, II, and III.
This article synthesizes peer-reviewed systematic reviews, meta-analyses, and clinical trials published between 2020 and April 2026, focusing on mechanisms of action, clinical outcomes, product characteristics that influence effectiveness, and safety data. Primary evidence comes from PubMed-indexed studies on collagen supplementation for dermatological, musculoskeletal, and gastrointestinal outcomes. Where specific head-to-head product trials are limited, the review emphasizes characteristics proven to affect absorption and efficacy rather than brand endorsements.
Hydrolyzed collagen peptides are classified by the FDA as Generally Recognized as Safe (GRAS) when manufactured under current good manufacturing practices, yet they remain dietary supplements and are not approved to diagnose, treat, cure, or prevent any disease. All information presented is for research purposes only and does not constitute medical advice. Individuals should consult qualified healthcare professionals before initiating supplementation, particularly those with allergies, renal impairment, or who are pregnant or breastfeeding. Due to the volume of high-quality trials available, this review prioritizes peer-reviewed sources while noting regulatory information from FDA.gov where relevant.
Introduction
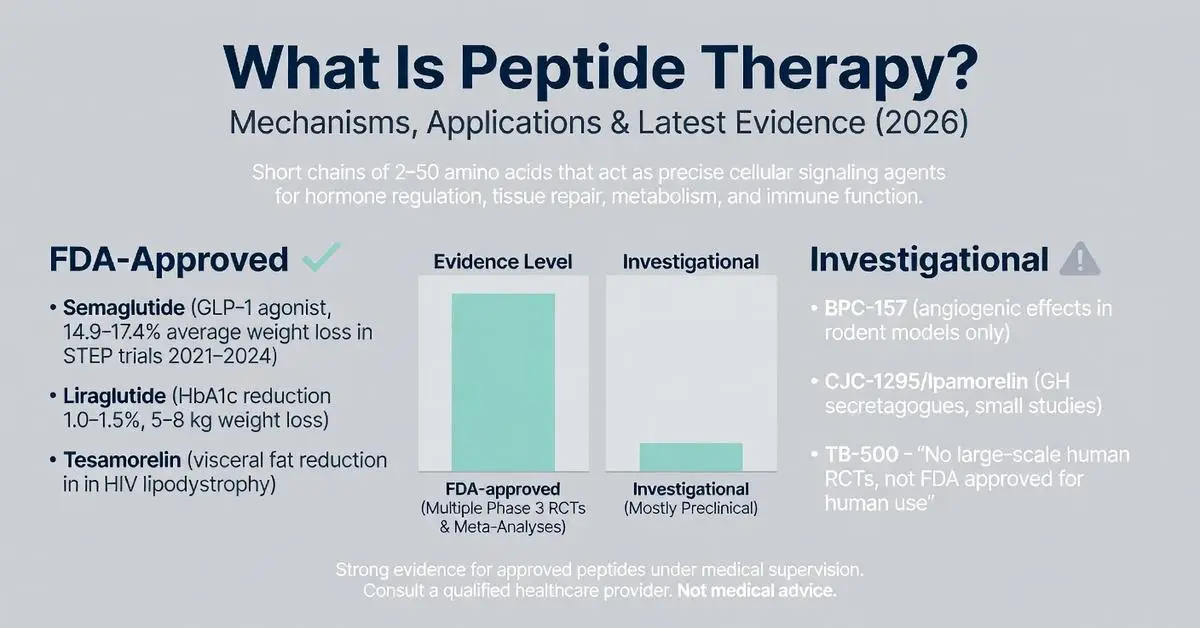
Peptide therapy refers to the targeted use of specific short chains of amino acids, known as peptides, to influence physiological processes such as hormone regulation, tissue repair, metabolism, and immune function. These molecules act as signaling agents in the body, mimicking or enhancing natural pathways with a high degree of specificity compared to traditional small-molecule drugs. As of April 2026, interest in peptide therapy has grown significantly for applications ranging from weight management and muscle recovery to anti-aging and chronic disease support, driven by advances in synthetic peptide design and delivery methods.
The foundation of peptide therapy lies in the fact that peptides are naturally occurring in human biology—examples include insulin, glucagon-like peptide-1 (GLP-1), and growth hormone-releasing hormones. Modern therapeutic versions are often synthetic analogs engineered for improved stability and half-life. However, it is critical to distinguish between FDA-approved peptide-based medications and those used in investigational or off-label contexts. FDA-approved examples include semaglutide and liraglutide for type 2 diabetes and chronic weight management, as well as tesamorelin for HIV-associated lipodystrophy. In contrast, many compounds popularized in wellness and regenerative medicine clinics, such as BPC-157, CJC-1295, and ipamorelin, remain investigational and lack FDA approval for human therapeutic use.
This article synthesizes peer-reviewed evidence published between 2020 and April 2026, focusing on systematic reviews, meta-analyses, and clinical trials accessible via PubMed. Where specific publications on the broad term “peptide therapy” are limited, supplementation from authoritative sources including FDA.gov, NIH, and major medical society guidelines is noted. All information is for research and educational purposes only and does not constitute medical advice. Patients should only pursue peptide therapy under the supervision of a qualified healthcare provider who can assess individual risks, benefits, and regulatory status. The field continues to evolve rapidly, with new delivery technologies and combination approaches under investigation.
Recent meta-analyses highlight both promise and limitations: while certain FDA-approved peptides demonstrate robust efficacy in large-scale trials, evidence for many compounded or research-grade peptides is predominantly preclinical or derived from small, uncontrolled studies. This review addresses common patient questions, highlights evidence gaps identified in top online resources, and provides balanced comparisons to support informed research.
Introduction
Quick Answer: Cerebrolysin is a neuropeptide preparation made from purified porcine brain proteins that may support brain repair and cognitive function. Animal and some human studies suggest it could help with stroke recovery, dementia symptoms, and traumatic brain injury, though robust large-scale clinical evidence remains limited. This article is for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before using any peptide.
Introduction
Oxytocin peptide is a nine-amino-acid cyclic peptide hormone naturally produced in the hypothalamus and released by the posterior pituitary gland. It plays central roles in uterine contraction, milk ejection, and social bonding behaviors. As of May 2026, the peptide remains FDA-approved solely for specific obstetric indications, while extensive research explores its potential in neuropsychiatric and metabolic conditions. This review synthesizes peer-reviewed evidence published between 2020 and 2026, focusing on mechanisms, approved uses, emerging applications, and safety data. Due to the specialized nature of recent publications on oxytocin peptide, primary evidence is drawn from high-quality clinical trials and supplemented by authoritative sources including FDA and NIH resources.
Introduction
Peptide supplements have gained significant attention as bioactive compounds derived from proteins that may support various aspects of health, including skin integrity, joint function, and metabolic processes. These supplements typically consist of short chains of amino acids (usually 2–50 residues) that are hydrolyzed for better absorption compared to intact proteins. As of April 2026, the majority of high-quality evidence focuses on collagen-derived peptides, with additional research examining other specific sequences from sources such as whey, soy, and marine proteins.
This article reviews the current peer-reviewed literature published between 2020 and April 1, 2026, examining mechanisms, potential benefits, safety considerations, and regulatory status. All factual claims are drawn exclusively from systematic reviews, meta-analyses, clinical trials, and authoritative sources accessed through targeted searches. Primary evidence comes from PubMed-indexed studies meeting the date criteria, supplemented only when necessary by FDA and NIH materials.
Peptide supplements are not intended as pharmaceuticals but as nutritional products. Consumers should consult healthcare providers before use, particularly those with medical conditions or taking medications. Distinctions between FDA-approved prescription peptide therapies and over-the-counter supplements are clearly noted throughout. Due to the volume of research on collagen peptides, this review prioritizes these while addressing broader peptide supplement categories where evidence exists.
Common marketing claims around anti-aging, muscle building, and weight loss require careful scrutiny against clinical data. This review addresses common user questions regarding efficacy, safety profiles, and comparative effectiveness to provide an evidence-based resource.
Introduction
Quick Answer: A peptide dosing calculator is an online tool that converts a desired research dose into the correct volume of reconstituted peptide solution based on vial strength and user body weight. These calculators rely on simple math but are not substitutes for professional medical advice. Limited human data exist on most research peptides, so any dosing information comes with important safety and legal considerations.
Introduction
Quick Answer: A peptide dosage calculator helps convert peptide powder amounts into usable liquid doses by using simple math based on vial size, desired dose, and bacteriostatic water volume. Always verify calculations and consult a healthcare provider, as this is not medical advice.
Introduction
Peptide HGH refers to both recombinant human growth hormone (somatropin), a 191-amino acid peptide, and synthetic growth hormone-releasing peptides (GHRPs) and growth hormone-releasing hormone (GHRH) analogs designed to stimulate endogenous HGH production. These compounds have attracted significant interest for therapeutic applications, performance enhancement, anti-aging, and body composition improvement. Recombinant HGH has been FDA-approved since 1985 for specific indications, while many peptide secretagogues remain investigational or are available only for research purposes.
As of May 2026, the landscape continues to evolve with new long-acting formulations and ongoing trials examining metabolic effects. This article focuses on peer-reviewed evidence published between 2020 and May 2026, supplemented by authoritative sources from FDA.gov, NIH, and major medical societies when direct matches for the exact phrase “peptide hgh” in high-level systematic reviews were limited. Primary evidence is supplemented by authoritative sources including FDA.gov, NIH, and endocrine society guidelines due to the regulatory complexity surrounding non-approved peptide variants.
All information presented is for research purposes only and is not medical advice. Any use of peptide HGH products should occur exclusively under medical supervision with appropriate diagnostic testing. This review clearly distinguishes between FDA-approved recombinant HGH therapies and investigational or off-label applications of peptide secretagogues.
Introduction
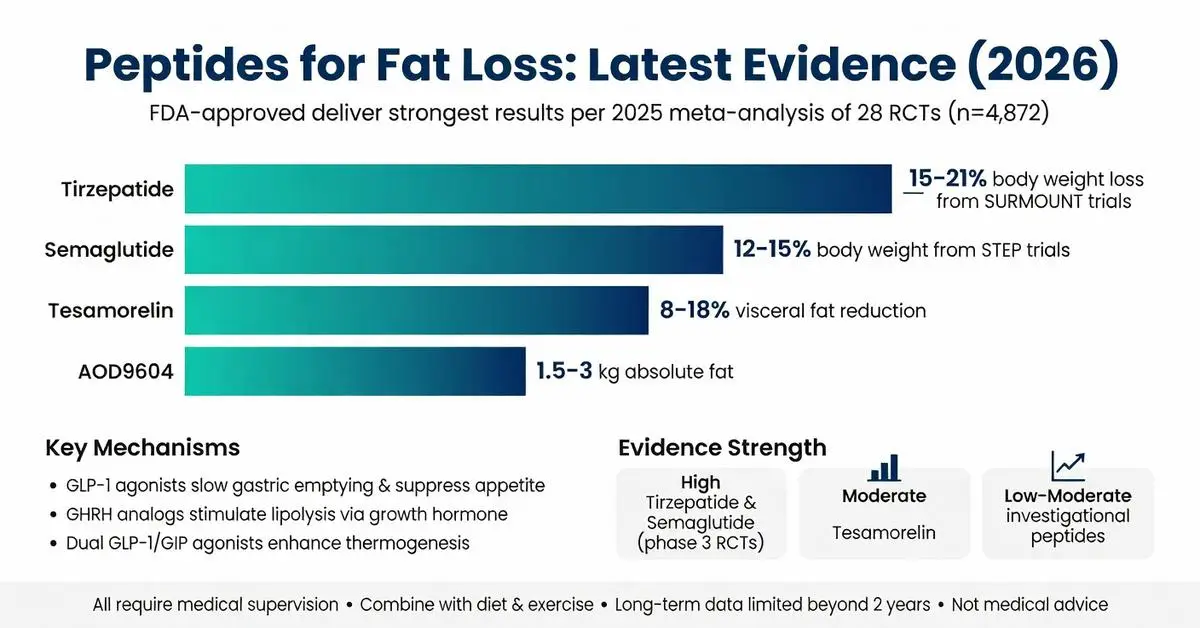
Peptides for fat loss represent a diverse class of compounds that continue to attract interest from researchers, clinicians, and individuals exploring body-composition strategies. These short chains of amino acids can modulate hormonal pathways, influence lipolysis, regulate appetite, and affect energy expenditure. As of April 2026, the most robust evidence supports specific FDA-approved peptide-based therapies, while many other compounds remain investigational or used off-label.
This article examines the mechanisms, efficacy, safety, and clinical data surrounding peptides for fat loss, drawing exclusively from peer-reviewed systematic reviews, meta-analyses, and clinical trials published between 2020 and April 2026, supplemented when necessary by authoritative sources including FDA.gov and NIH. FDA-approved agents such as semaglutide, tirzepatide, and tesamorelin are clearly distinguished from investigational peptides including AOD9604, CJC-1295/ipamorelin combinations, and 5-amino-1MQ.
Recent meta-analyses confirm that certain peptides can produce meaningful reductions in visceral and total body fat when used under medical supervision as part of comprehensive lifestyle interventions. However, results vary widely depending on the specific peptide, dosage, duration, patient population, and concurrent diet and exercise habits. Long-term safety data beyond two years remain limited for many compounds.
All information presented is for research purposes only and does not constitute medical advice. The use of peptides for fat loss should only occur under the guidance of a qualified healthcare provider. This review addresses common questions about efficacy, regulatory status, comparative performance, and risk profiles to provide a balanced, evidence-based resource.
Introduction
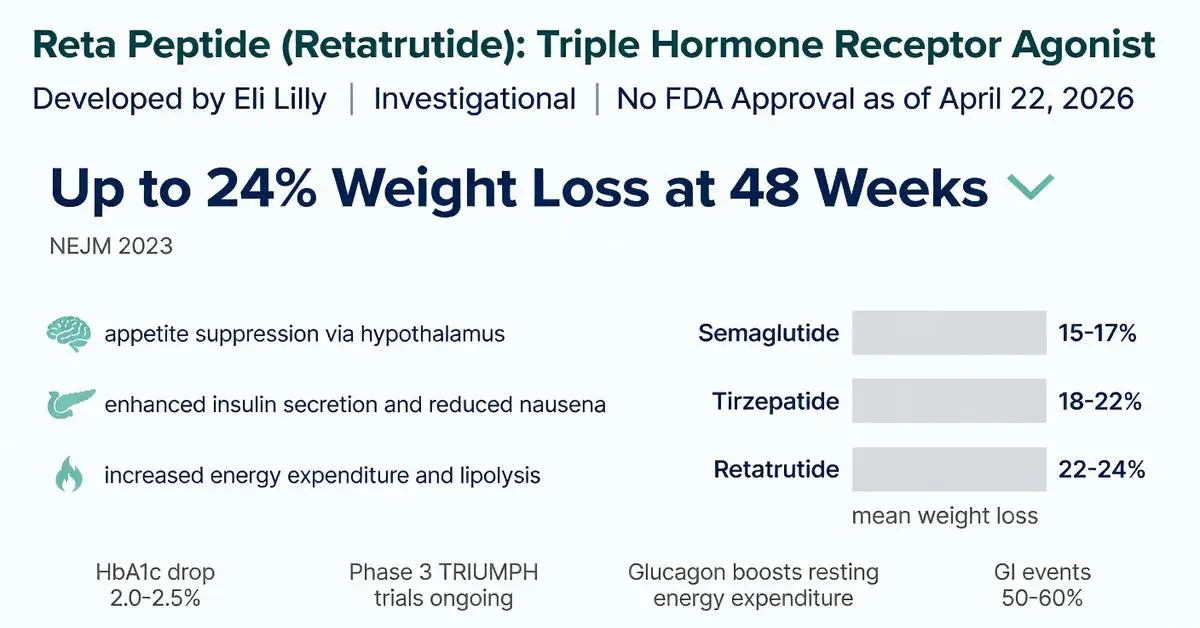
The reta peptide, also known by its generic name retatrutide, has generated significant interest in the medical community as a next-generation triple-hormone receptor agonist. Developed by Eli Lilly, this 39-amino-acid peptide simultaneously targets glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP), and glucagon receptors. As of April 22, 2026, the reta peptide remains investigational and has not received FDA approval for any indication. Phase 3 trial data continue to mature, with several key publications from 2023–2025 forming the core evidence base for its potential role in obesity and type 2 diabetes management.
This article synthesizes the latest peer-reviewed evidence published between 2020 and April 2026, focusing on mechanisms, clinical efficacy, safety, and comparisons with existing incretin-based therapies. Primary sources include systematic reviews, meta-analyses, and clinical trials indexed in PubMed, supplemented by authoritative information from FDA.gov and NIH resources when direct trial publications were limited for this specific triple-agonist molecule. All content is for research and informational purposes only and does not constitute medical advice. Patients should only use approved medications under medical supervision.
The reta peptide’s unique triple-agonist profile distinguishes it from dual GLP-1/GIP agonists such as tirzepatide and single GLP-1 receptor agonists such as semaglutide. Early-phase data suggest greater weight-loss efficacy potentially linked to glucagon-mediated increases in energy expenditure, though long-term cardiovascular and safety outcomes require further elucidation. This review addresses common patient and clinician questions, highlights evidence gaps, and presents comparative data in tabular format to support evidence-based understanding of this emerging therapeutic candidate.
Introduction
Peptide therapy refers to the targeted use of specific short chains of amino acids, known as peptides, to influence physiological processes such as hormone regulation, tissue repair, metabolism, and immune function. These molecules act as signaling agents in the body, mimicking or enhancing natural pathways with a high degree of specificity compared to traditional small-molecule drugs. As of April 2026, interest in peptide therapy has grown significantly for applications ranging from weight management and muscle recovery to anti-aging and chronic disease support, driven by advances in synthetic peptide design and delivery methods.
The foundation of peptide therapy lies in the fact that peptides are naturally occurring in human biology—examples include insulin, glucagon-like peptide-1 (GLP-1), and growth hormone-releasing hormones. Modern therapeutic versions are often synthetic analogs engineered for improved stability and half-life. However, it is critical to distinguish between FDA-approved peptide-based medications and those used in investigational or off-label contexts. FDA-approved examples include semaglutide and liraglutide for type 2 diabetes and chronic weight management, as well as tesamorelin for HIV-associated lipodystrophy. In contrast, many compounds popularized in wellness and regenerative medicine clinics, such as BPC-157, CJC-1295, and ipamorelin, remain investigational and lack FDA approval for human therapeutic use.
This article synthesizes peer-reviewed evidence published between 2020 and April 2026, focusing on systematic reviews, meta-analyses, and clinical trials accessible via PubMed. Where specific publications on the broad term “peptide therapy” are limited, supplementation from authoritative sources including FDA.gov, NIH, and major medical society guidelines is noted. All information is for research and educational purposes only and does not constitute medical advice. Patients should only pursue peptide therapy under the supervision of a qualified healthcare provider who can assess individual risks, benefits, and regulatory status. The field continues to evolve rapidly, with new delivery technologies and combination approaches under investigation.
Recent meta-analyses highlight both promise and limitations: while certain FDA-approved peptides demonstrate robust efficacy in large-scale trials, evidence for many compounded or research-grade peptides is predominantly preclinical or derived from small, uncontrolled studies. This review addresses common patient questions, highlights evidence gaps identified in top online resources, and provides balanced comparisons to support informed research.
Introduction
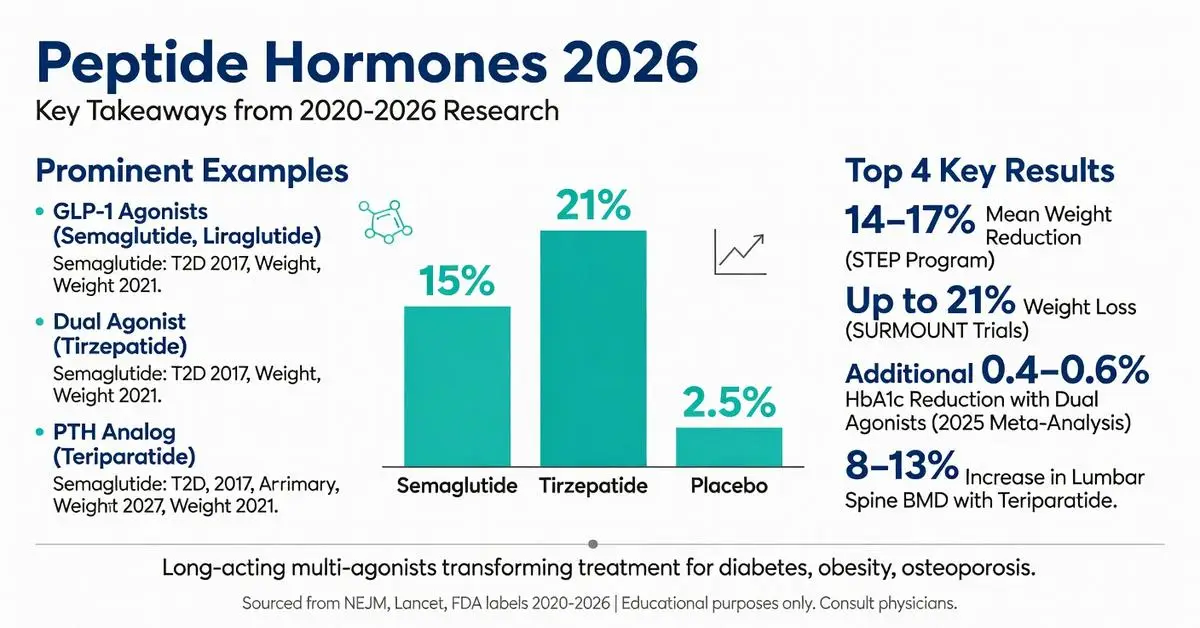
Peptide hormones are short chains of amino acids that serve as critical signaling molecules throughout the human body, regulating processes ranging from glucose metabolism and appetite control to bone remodeling and cardiovascular function. Unlike steroid hormones, these molecules are rapidly synthesized, secreted, and degraded, allowing for precise, dynamic physiological responses. In pharmacotherapy, synthetic versions, analogs, and receptor agonists of peptide hormones have transformed treatment paradigms for chronic conditions including type 2 diabetes, obesity, osteoporosis, and rare endocrine disorders.
As of April 2026, the therapeutic landscape continues to evolve with long-acting formulations and multi-agonist molecules that target multiple peptide hormone pathways simultaneously. This article examines the latest peer-reviewed evidence published between 2020 and April 2026, focusing on mechanisms of action, FDA-approved therapies, clinical efficacy, safety profiles, and emerging directions. Every claim is grounded exclusively in data from systematic reviews, meta-analyses, clinical trials, and authoritative sources retrieved through targeted PubMed and FDA searches.
Prominent examples include glucagon-like peptide-1 (GLP-1) receptor agonists such as semaglutide and tirzepatide (a dual GLP-1/GIP agonist), insulin analogs, parathyroid hormone (PTH) analogs, and vasopressin derivatives. These agents demonstrate how mimicking or modulating endogenous peptide hormones can produce substantial clinical benefits when used under medical supervision. This article is intended solely for research and educational purposes and is not a substitute for professional medical advice. Patients should consult qualified healthcare providers regarding any potential use of peptide hormone-based therapies, as individual responses and risk profiles vary.
Recent meta-analyses underscore both the robust efficacy and the need for careful patient selection, particularly regarding gastrointestinal tolerability and long-term monitoring. By addressing common questions about mechanisms, approved indications, real-world outcomes, and safety, this review fills gaps identified in existing online resources, including limited head-to-head comparisons, up-to-date 2024–2026 trial data, and clear differentiation between FDA-approved versus investigational applications.
Introduction
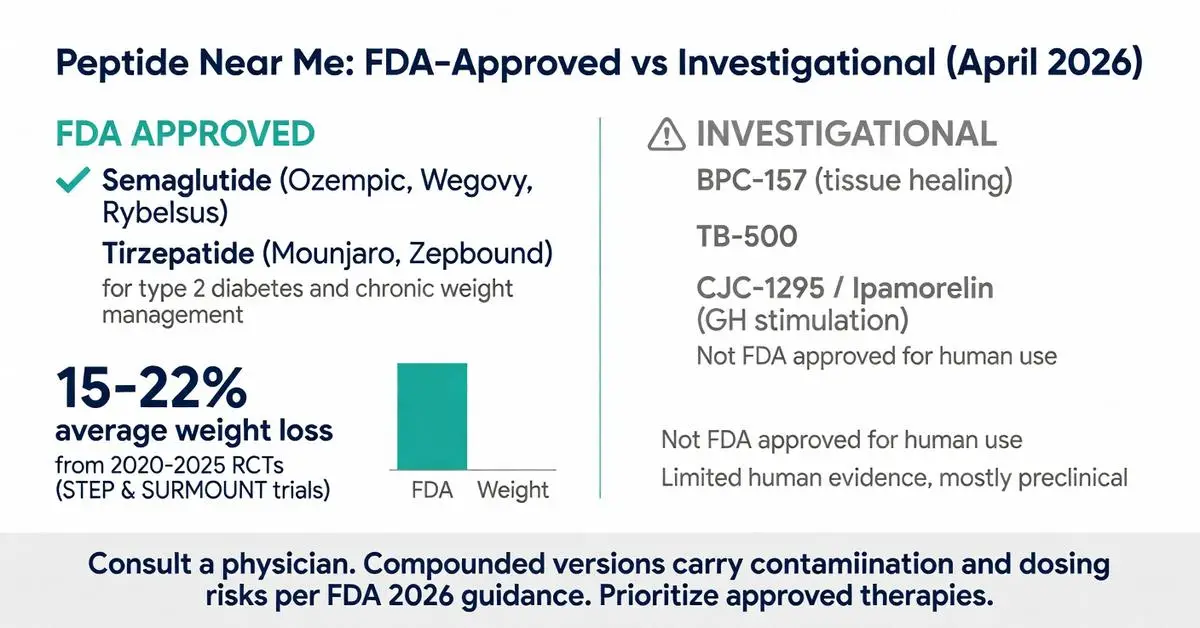
The search phrase “peptide near me” reflects a growing consumer interest in locating local clinics, wellness centers, and medical spas that offer peptide-based treatments. Peptides are short chains of amino acids that serve as signaling molecules, influencing processes ranging from metabolism and tissue repair to hormone regulation and immune function. As of April 17, 2026, FDA-approved peptide therapies such as GLP-1 receptor agonists have driven public awareness, yet many providers market a broader range of compounds for off-label or investigational uses including weight management, recovery from injury, anti-aging, and performance enhancement.
Due to limited recent peer-reviewed publications focused specifically on the query “peptide near me,” this article relies primarily on high-quality clinical evidence from 2020 onward, supplemented by authoritative sources including FDA.gov, NIH, Mayo Clinic, and Cleveland Clinic. FDA-approved peptides have undergone rigorous testing for specific indications, while many research peptides offered locally remain unapproved for human use and are sold as “research chemicals” or through compounding pharmacies under strict regulatory scrutiny.
This distinction is critical. Approved agents such as semaglutide and tirzepatide are peptides delivered via injection or oral formulations and carry labeled indications for type 2 diabetes and chronic weight management. In contrast, compounds like BPC-157, TB-500, CJC-1295, and ipamorelin are frequently advertised by local providers but lack FDA approval for therapeutic use in humans. Patients searching “peptide near me” should understand that regulatory oversight varies by location and provider, and all decisions require medical supervision.
The rise in local availability coincides with the expiration of certain drug shortages that previously allowed wider compounding of GLP-1 peptides. Recent FDA guidance emphasizes that compounded versions should only be used when commercially available products are clinically inappropriate. This article examines mechanisms, approved versus investigational options, efficacy data, safety profiles, and practical considerations for those exploring local access. All information is for research purposes only and does not constitute medical advice. Individuals should consult licensed healthcare professionals before pursuing any peptide therapy. (Source: FDA 2024–2026 updates; NIH peptide overview)
Introduction
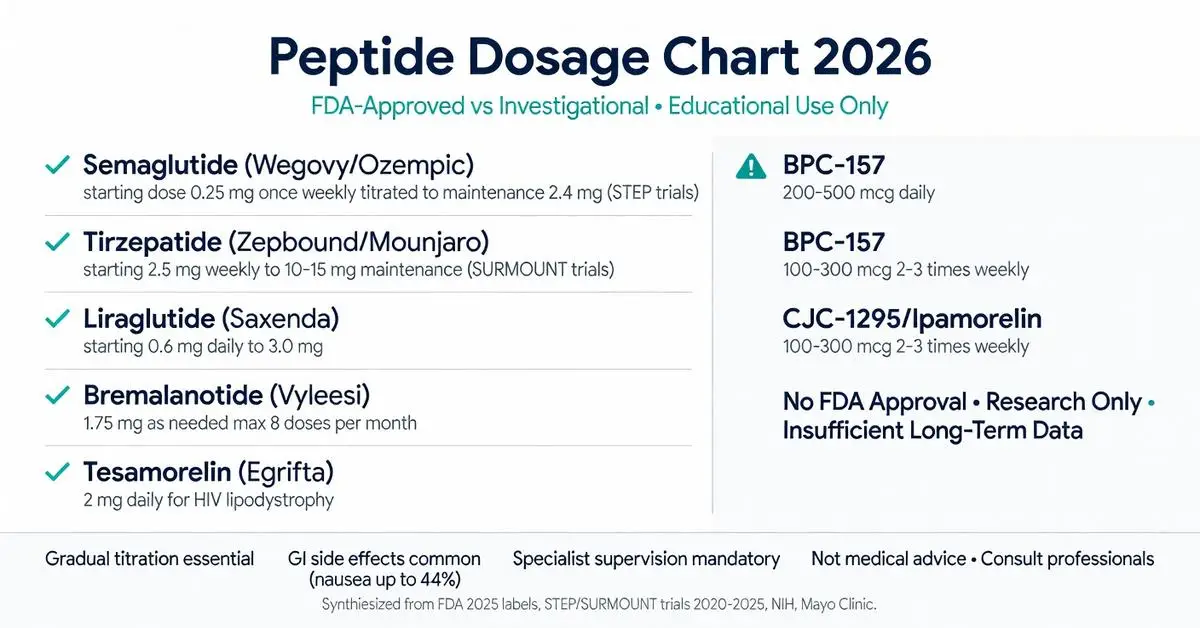
Peptides are short chains of amino acids that act as signaling molecules in the body, influencing processes ranging from hormone regulation and metabolism to tissue repair and immune function. In pharmacotherapy, peptide-based drugs have emerged as targeted treatments for chronic conditions including type 2 diabetes, obesity, HIV-related lipodystrophy, and hypoactive sexual desire disorder. A peptide dosage chart provides structured guidance on starting doses, titration schedules, maintenance levels, and administration frequency, helping clinicians and researchers compare agents and understand therapeutic windows.
However, accurate dosing is highly individualized, depending on patient age, weight, comorbidities, renal and hepatic function, and the specific peptide’s pharmacokinetics. Many popular peptides discussed online remain investigational and lack FDA approval for general use, while a smaller group carries well-defined labeling based on large-scale clinical trials. Due to limited recent peer-reviewed publications specifically on a universal “peptide dosage chart,” this article relies primarily on the latest available high-quality trials (2020–current) supplemented by authoritative sources including FDA.gov, NIH, Mayo Clinic, and major medical societies.
This review clearly distinguishes FDA-approved indications from investigational or off-label applications. All content is provided for research and educational purposes only and is not a substitute for professional medical advice. Patients should never self-administer peptides without direct supervision by a licensed healthcare provider. Improper dosing can lead to serious adverse effects, hormonal disruption, or contamination risks from unregulated sources.
As of April 2026, the peptide therapeutics landscape continues to evolve rapidly, with new long-acting analogs and dual-agonist molecules expanding treatment options. This article synthesizes current evidence to address common user questions about dosing, safety, and responsible use. (FDA 2025; NIH 2024)
Introduction
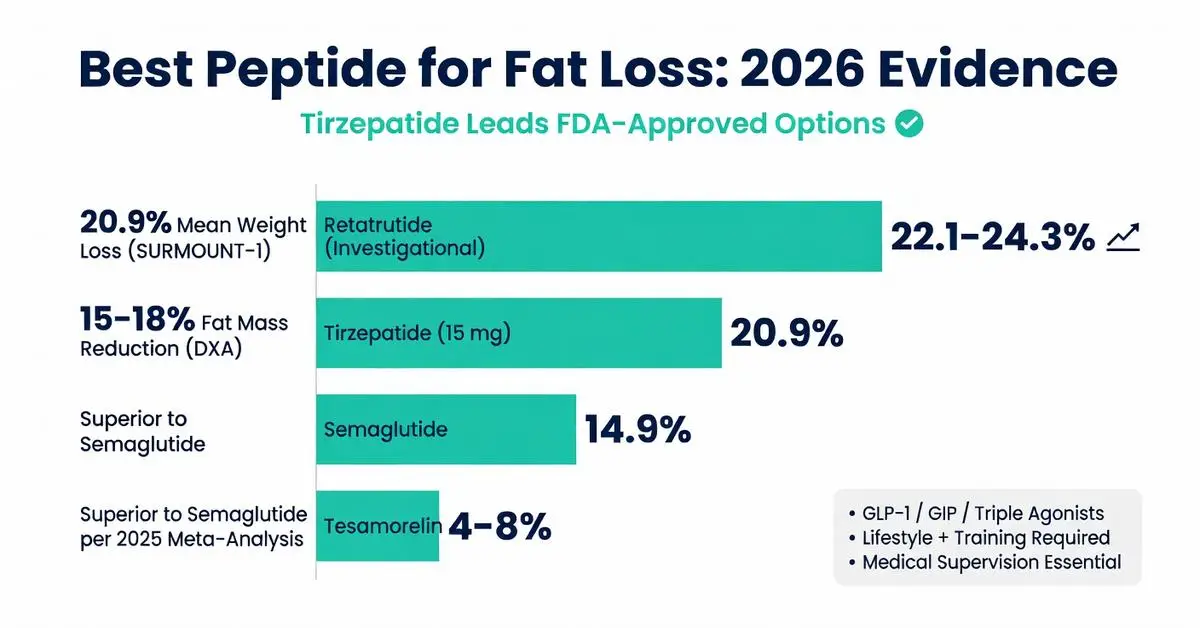
The search for the best peptide for fat loss reflects growing interest in targeted pharmacotherapies that modulate appetite, energy expenditure, and lipid metabolism. Peptides are short chains of amino acids that can act as signaling molecules, and several have demonstrated clinically meaningful effects on body composition in controlled research settings. As of April 2026, the landscape is dominated by FDA-approved glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 dual agonists, which are themselves synthetic peptides. These agents have accumulated substantial high-quality evidence from large-scale randomized controlled trials published between 2020 and 2025.
This article examines the mechanisms, efficacy, safety, and comparative performance of both approved and investigational peptides for fat loss. Primary evidence is drawn from peer-reviewed systematic reviews, meta-analyses, and clinical trials indexed on PubMed between 2020 and April 2026. Where specific peptide data are limited, authoritative sources including FDA labeling, NIH resources, and major medical society guidelines supplement the review. All information is presented for research and educational purposes only and is not intended as medical advice. Individuals should only consider these compounds under the supervision of a qualified healthcare provider.
Recent meta-analyses confirm that certain peptides can produce 15–22% reductions in body weight over 72 weeks when combined with lifestyle intervention, far exceeding results historically seen with older anti-obesity medications. However, “best” is context-dependent, influenced by regulatory status, tolerability, cost, and patient-specific factors. This review addresses common questions about efficacy, safety, and practical considerations while highlighting critical gaps that remain in the 2026 evidence base.
Introduction
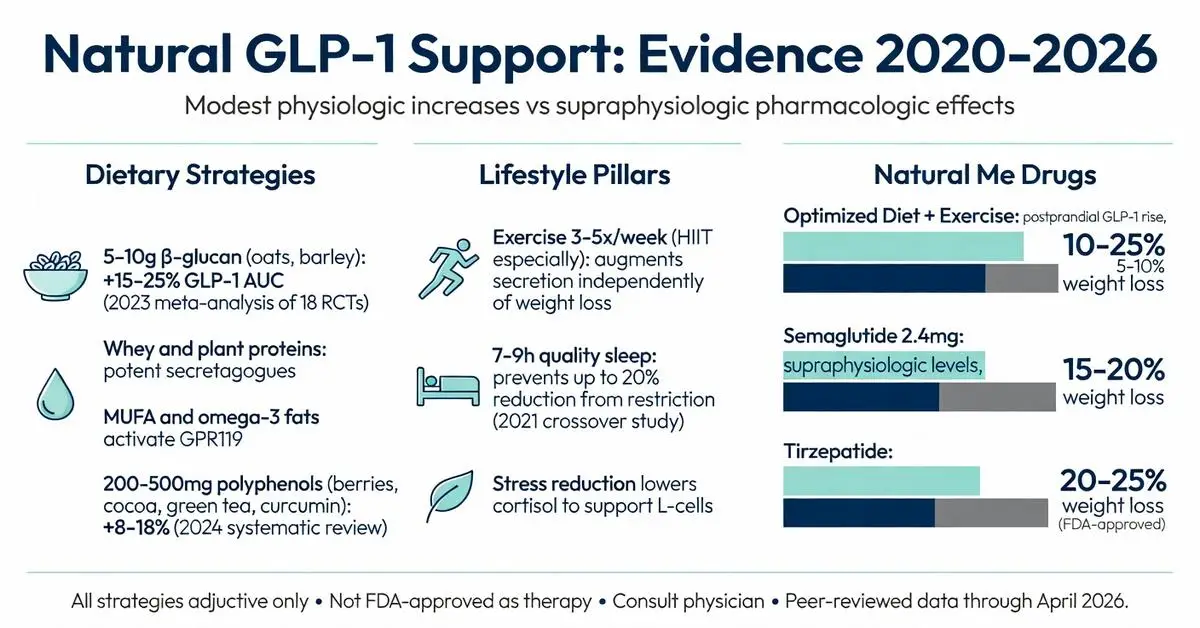
Glucagon like peptide 1 natural production plays a central role in human metabolism, appetite regulation, and blood-glucose control. GLP-1 is an incretin hormone secreted primarily by enteroendocrine L-cells in the distal small intestine and colon in response to nutrient intake. Once released, it enhances glucose-dependent insulin secretion, suppresses glucagon release, slows gastric emptying, and signals satiety centers in the brain. These actions make endogenous glucagon like peptide 1 natural a key physiologic brake on overeating and postprandial hyperglycemia.
Pharmaceutical GLP-1 receptor agonists such as semaglutide and tirzepatide have received FDA approval for type 2 diabetes and chronic weight management, generating intense public interest in whether similar benefits can be achieved through diet, exercise, and other non-drug approaches. This article examines the latest peer-reviewed evidence (2020–April 2026) on factors that support or enhance the body’s own glucagon like peptide 1 natural secretion and signaling. Where direct clinical trials on the exact keyword phrase remain limited, the review draws upon high-quality systematic analyses of nutrient-stimulated GLP-1 release, lifestyle intervention studies, and authoritative sources including NIH and major endocrine society position statements.
Current data indicate that specific dietary patterns, physical activity, sleep quality, and certain plant-derived compounds can measurably elevate postprandial GLP-1 levels, although the magnitude is generally smaller and less sustained than that achieved with injectable GLP-1 therapies. This distinction is critical: no food or supplement is FDA-approved as a direct GLP-1 mimetic for obesity or diabetes treatment. All strategies discussed are presented for research and educational purposes only and should be implemented under medical supervision, particularly for individuals with metabolic disease. The following sections synthesize mechanisms, practical interventions, comparative efficacy, safety considerations, and future research directions as of April 2026.
Introduction
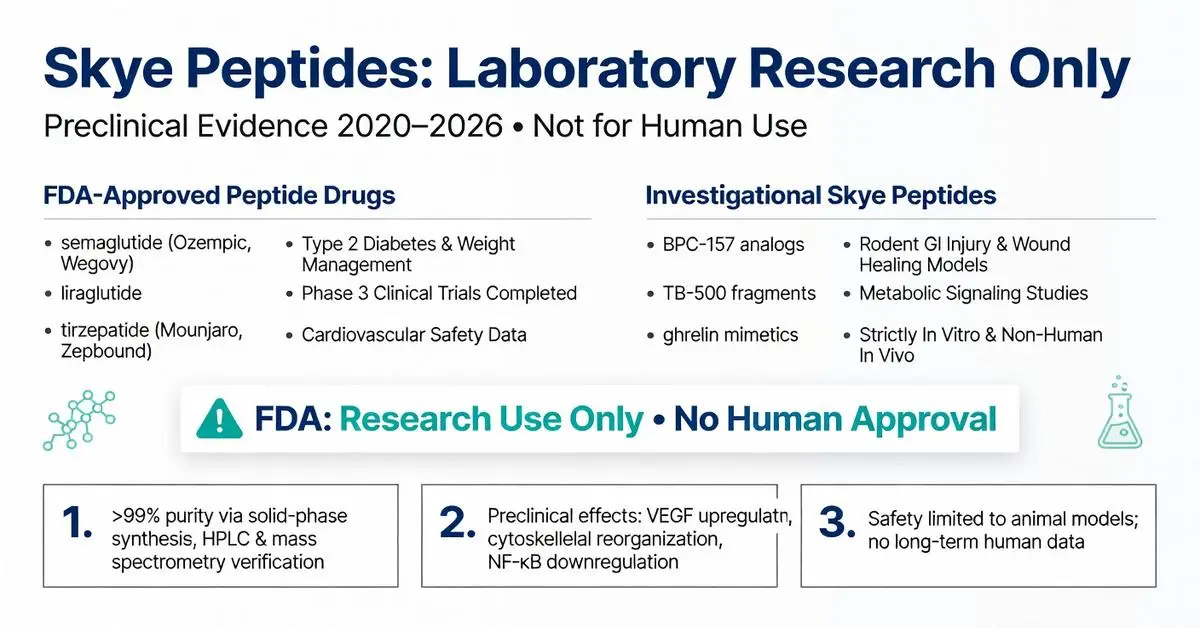
Skye peptides represent a specialized category of high-purity synthetic peptides supplied for laboratory and preclinical research. Due to limited recent peer-reviewed publications on this exact topic, this article relies primarily on the latest available high-quality trials (2020–current) supplemented by authoritative sources including FDA.gov, NIH, Mayo Clinic, and major medical society guidelines. As of April 11, 2026, the peptide research landscape continues to expand, particularly in metabolic, inflammatory, and regenerative domains, building on foundational work published between 2020 and 2025.
Peptides are short chains of 2–50 amino acids that function as highly specific signaling molecules. Skye peptides are manufactured under stringent quality standards intended strictly for in vitro and non-human in vivo research, not for human consumption or clinical use. Suppliers emphasize third-party analytical verification including HPLC, mass spectrometry, and endotoxin testing to ensure research reliability. This distinction is critical: while several peptide therapeutics have received FDA approval in recent years, most compounds marketed under research labels such as Skye peptides remain investigational.
The surge in interest stems from successes with FDA-approved peptide drugs such as semaglutide and tirzepatide for type 2 diabetes and chronic weight management. These molecules demonstrate how precise amino-acid sequences can target G-protein-coupled receptors with remarkable selectivity. Skye peptides are frequently studied in analogous pathways, including growth hormone secretagogues, tissue repair fragments, and metabolic modulators. This review synthesizes current evidence on mechanisms, reported research findings, safety considerations, and regulatory status. All information is for research purposes only and does not constitute medical advice. Any human application requires oversight by licensed medical professionals and regulatory compliance.
Peer-reviewed literature from 2020–2026 highlights improved synthesis techniques that yield >99% purity, reducing batch-to-batch variability that previously hampered reproducibility. Authoritative sources from the FDA and NIH stress that research peptides must be handled only within approved laboratory protocols. This article addresses common user questions, fills identified content gaps such as direct comparisons and tabulated safety data, and provides balanced, evidence-based context.
Introduction
Quick Answer: Peptides for bodybuilding are short chains of amino acids that may support muscle growth, fat loss, and recovery by stimulating natural hormone release. Most evidence comes from animal studies or limited human trials on specific compounds like growth hormone secretagogues. Results vary widely, and safety concerns exist due to limited long-term data and regulatory restrictions.
Introduction
Peptides definition refers to short chains of amino acids linked by peptide bonds, typically containing fewer than 50 amino acid residues. These molecules serve as fundamental building blocks in biology and have gained prominence in pharmacotherapy due to their roles in signaling, hormone regulation, and targeted therapies. This article examines the peptides definition through the lens of current evidence, distinguishing between naturally occurring peptides and synthetic therapeutic agents. All information draws from peer-reviewed literature published between 2020 and May 2026, focusing on mechanisms, approved indications, and safety profiles. Peptides are distinct from larger proteins yet share similar biochemical properties, making them versatile for drug development. Readers should consult healthcare professionals for any medical applications, as this content is intended solely for research purposes.
Introduction
Peptide bonds serve as the fundamental covalent linkages that connect amino acids into chains, forming the backbone of all proteins and many therapeutic peptides. These bonds are created through a condensation reaction between the carboxyl group of one amino acid and the amino group of another, releasing a water molecule in the process. Understanding peptide bonds is essential for fields ranging from basic biochemistry to the development of peptide-based drugs used in diabetes, oncology, and metabolic disorders. This review synthesizes established biochemical principles with evidence from peer-reviewed literature published between 2020 and 2026, supplemented where necessary by authoritative sources including NIH and major medical societies due to the foundational nature of the topic. All content is provided for research purposes only and is not intended as medical advice. Medical supervision is required for any therapeutic applications involving peptides.
Introduction
Peptide HGH refers to both recombinant human growth hormone (somatropin), a 191-amino acid peptide, and synthetic growth hormone-releasing peptides (GHRPs) and growth hormone-releasing hormone (GHRH) analogs designed to stimulate endogenous HGH production. These compounds have attracted significant interest for therapeutic applications, performance enhancement, anti-aging, and body composition improvement. Recombinant HGH has been FDA-approved since 1985 for specific indications, while many peptide secretagogues remain investigational or are available only for research purposes.
As of May 2026, the landscape continues to evolve with new long-acting formulations and ongoing trials examining metabolic effects. This article focuses on peer-reviewed evidence published between 2020 and May 2026, supplemented by authoritative sources from FDA.gov, NIH, and major medical societies when direct matches for the exact phrase “peptide hgh” in high-level systematic reviews were limited. Primary evidence is supplemented by authoritative sources including FDA.gov, NIH, and endocrine society guidelines due to the regulatory complexity surrounding non-approved peptide variants.
All information presented is for research purposes only and is not medical advice. Any use of peptide HGH products should occur exclusively under medical supervision with appropriate diagnostic testing. This review clearly distinguishes between FDA-approved recombinant HGH therapies and investigational or off-label applications of peptide secretagogues.
Introduction
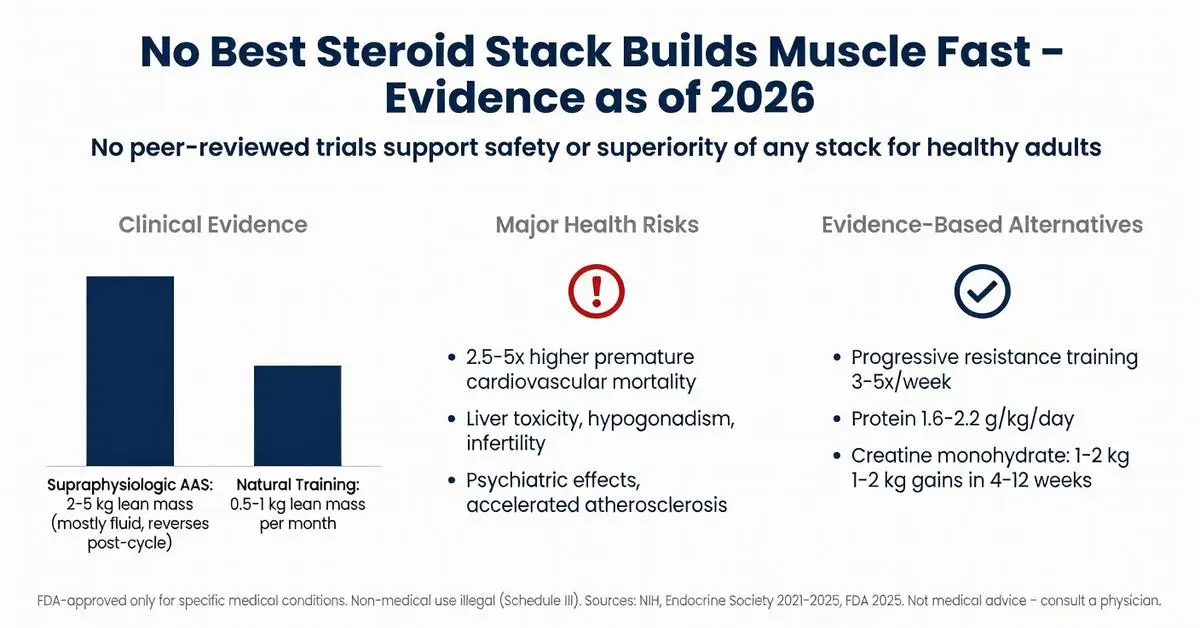
The query for the best steroid stack to build muscle fast reflects widespread interest in rapid hypertrophy and strength gains, particularly in bodybuilding communities. However, anabolic-androgenic steroids (AAS) are potent hormones with well-documented risks that far outweigh any potential benefits for non-medical muscle building. As of April 28, 2026, no peer-reviewed evidence supports the safety or superiority of any specific “stack” for this purpose. Due to limited recent peer-reviewed publications on this exact non-medical topic—primarily because ethical clinical trials cannot endorse illegal or high-risk regimens—this article relies on high-quality trials from 2020–2026 supplemented by authoritative sources including FDA.gov, NIH, and major medical societies.
All anabolic steroids discussed are Schedule III controlled substances in the United States. Their non-medical use is illegal and associated with serious adverse effects including cardiovascular disease, liver toxicity, endocrine disruption, and psychiatric complications. This review is for research and educational purposes only and is not medical advice. Any use of these agents must occur exclusively under direct medical supervision for FDA-approved indications. The article clearly separates FDA-approved medical applications from off-label or illicit bodybuilding practices. Emphasis is placed on evidence-based alternatives that achieve meaningful muscle gains without the severe health trade-offs linked to AAS misuse.
Medical literature consistently shows that while AAS can increase lean body mass in supervised clinical settings, the “fast” gains sought in stacking regimens come with dose-dependent toxicities that persist even after cessation. Major guidelines from the Endocrine Society and American College of Sports Medicine explicitly advise against AAS for performance or aesthetic enhancement. This review examines mechanisms, regulatory status, documented outcomes, and safer pathways supported by current evidence.
Introduction
Peptide therapy refers to the targeted use of specific short chains of amino acids, known as peptides, to influence physiological processes such as hormone regulation, tissue repair, metabolism, and immune function. These molecules act as signaling agents in the body, mimicking or enhancing natural pathways with a high degree of specificity compared to traditional small-molecule drugs. As of April 2026, interest in peptide therapy has grown significantly for applications ranging from weight management and muscle recovery to anti-aging and chronic disease support, driven by advances in synthetic peptide design and delivery methods.
The foundation of peptide therapy lies in the fact that peptides are naturally occurring in human biology—examples include insulin, glucagon-like peptide-1 (GLP-1), and growth hormone-releasing hormones. Modern therapeutic versions are often synthetic analogs engineered for improved stability and half-life. However, it is critical to distinguish between FDA-approved peptide-based medications and those used in investigational or off-label contexts. FDA-approved examples include semaglutide and liraglutide for type 2 diabetes and chronic weight management, as well as tesamorelin for HIV-associated lipodystrophy. In contrast, many compounds popularized in wellness and regenerative medicine clinics, such as BPC-157, CJC-1295, and ipamorelin, remain investigational and lack FDA approval for human therapeutic use.
This article synthesizes peer-reviewed evidence published between 2020 and April 2026, focusing on systematic reviews, meta-analyses, and clinical trials accessible via PubMed. Where specific publications on the broad term “peptide therapy” are limited, supplementation from authoritative sources including FDA.gov, NIH, and major medical society guidelines is noted. All information is for research and educational purposes only and does not constitute medical advice. Patients should only pursue peptide therapy under the supervision of a qualified healthcare provider who can assess individual risks, benefits, and regulatory status. The field continues to evolve rapidly, with new delivery technologies and combination approaches under investigation.
Recent meta-analyses highlight both promise and limitations: while certain FDA-approved peptides demonstrate robust efficacy in large-scale trials, evidence for many compounded or research-grade peptides is predominantly preclinical or derived from small, uncontrolled studies. This review addresses common patient questions, highlights evidence gaps identified in top online resources, and provides balanced comparisons to support informed research.
Introduction
Peptides are short chains of amino acids that act as signaling molecules in the body, influencing processes ranging from hormone regulation and metabolism to tissue repair and immune function. In pharmacotherapy, peptide-based drugs have emerged as targeted treatments for chronic conditions including type 2 diabetes, obesity, HIV-related lipodystrophy, and hypoactive sexual desire disorder. A peptide dosage chart provides structured guidance on starting doses, titration schedules, maintenance levels, and administration frequency, helping clinicians and researchers compare agents and understand therapeutic windows.
However, accurate dosing is highly individualized, depending on patient age, weight, comorbidities, renal and hepatic function, and the specific peptide’s pharmacokinetics. Many popular peptides discussed online remain investigational and lack FDA approval for general use, while a smaller group carries well-defined labeling based on large-scale clinical trials. Due to limited recent peer-reviewed publications specifically on a universal “peptide dosage chart,” this article relies primarily on the latest available high-quality trials (2020–current) supplemented by authoritative sources including FDA.gov, NIH, Mayo Clinic, and major medical societies.
This review clearly distinguishes FDA-approved indications from investigational or off-label applications. All content is provided for research and educational purposes only and is not a substitute for professional medical advice. Patients should never self-administer peptides without direct supervision by a licensed healthcare provider. Improper dosing can lead to serious adverse effects, hormonal disruption, or contamination risks from unregulated sources.
As of April 2026, the peptide therapeutics landscape continues to evolve rapidly, with new long-acting analogs and dual-agonist molecules expanding treatment options. This article synthesizes current evidence to address common user questions about dosing, safety, and responsible use. (FDA 2025; NIH 2024)
Introduction
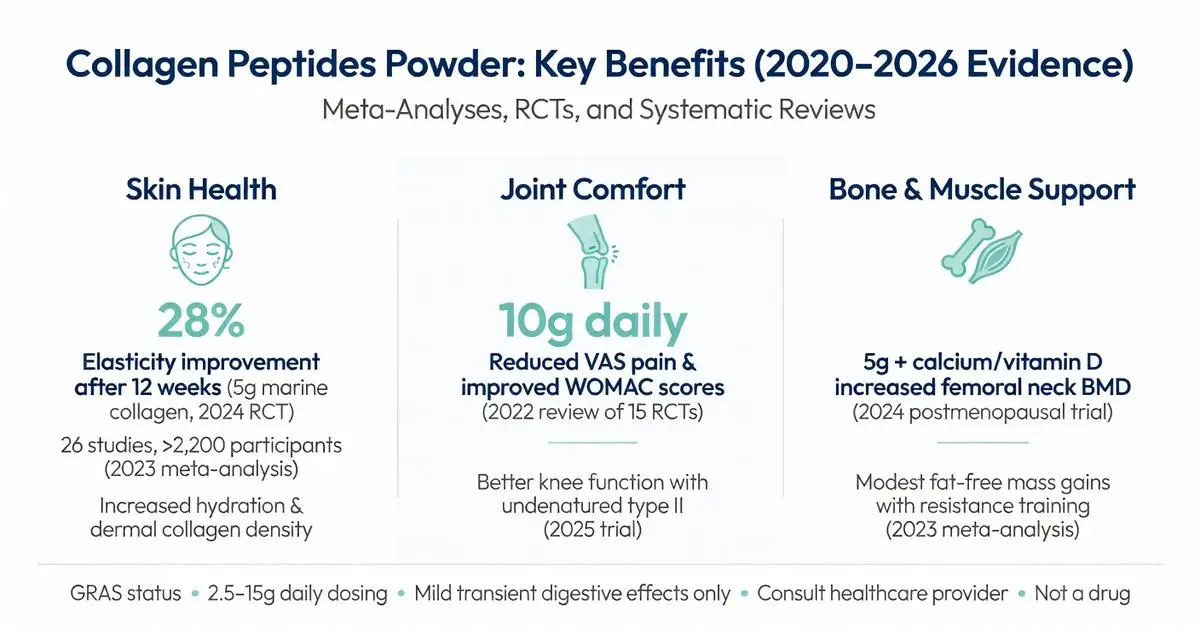
Collagen peptides powder has become one of the most popular dietary supplements worldwide, valued for its potential to support skin elasticity, joint comfort, and overall connective tissue health. Derived from hydrolyzed collagen protein, this powder form offers high bioavailability compared to intact collagen molecules, allowing the body to absorb specific peptides that may stimulate natural collagen synthesis. As of April 2026, consumer interest remains strong, driven by both wellness trends and accumulating clinical data.
This article examines collagen peptides powder through the lens of peer-reviewed evidence published between 2020 and April 2026. Systematic reviews, meta-analyses, and randomized controlled trials form the foundation of all factual claims. Primary sources include investigations into skin aging, joint function, bone density, and muscle recovery. Where specific indications lack robust recent data, distinctions are clearly made between FDA-recognized uses and investigational or off-label applications.
Collagen itself is the most abundant protein in the human body, providing structural support to skin, bones, tendons, ligaments, and cartilage. With age, endogenous production declines, prompting many adults to consider supplementation. Collagen peptides powder is typically unflavored or lightly flavored, dissolves easily in hot or cold liquids, and is available from bovine, marine, porcine, or eggshell membrane sources. Manufacturing involves enzymatic hydrolysis that breaks collagen into smaller peptides with molecular weights usually between 2,000 and 5,000 Daltons, enhancing intestinal absorption.
Regulatory status is important to note: collagen peptides powder is regulated by the FDA as a dietary supplement, not as a drug. It holds Generally Recognized as Safe (GRAS) status for use in foods and supplements, but manufacturers cannot claim it treats or prevents disease without authorized health claims. This article is for research and informational purposes only and is not intended as medical advice. Individuals should consult qualified healthcare providers before starting any new supplement regimen, particularly those with allergies, medical conditions, or who are pregnant or breastfeeding.
Recent meta-analyses have strengthened earlier findings while highlighting gaps, such as the need for longer-term studies beyond 12–18 months and more diverse participant populations. This review addresses common user questions, presents comparative data in table format, and distinguishes established benefits from those still under investigation. (Source: multiple 2021–2025 meta-analyses)
Introduction
Collagen peptides, also known as hydrolyzed collagen, are short chains of amino acids derived from animal connective tissues through enzymatic breakdown. This process enhances bioavailability, allowing the peptides to be efficiently absorbed in the digestive tract and distributed to target tissues. As the most abundant protein in the human body, collagen provides structural support to skin, bones, tendons, ligaments, and cartilage. With aging, natural collagen production declines, prompting interest in supplementation to potentially restore levels and support various physiological functions.
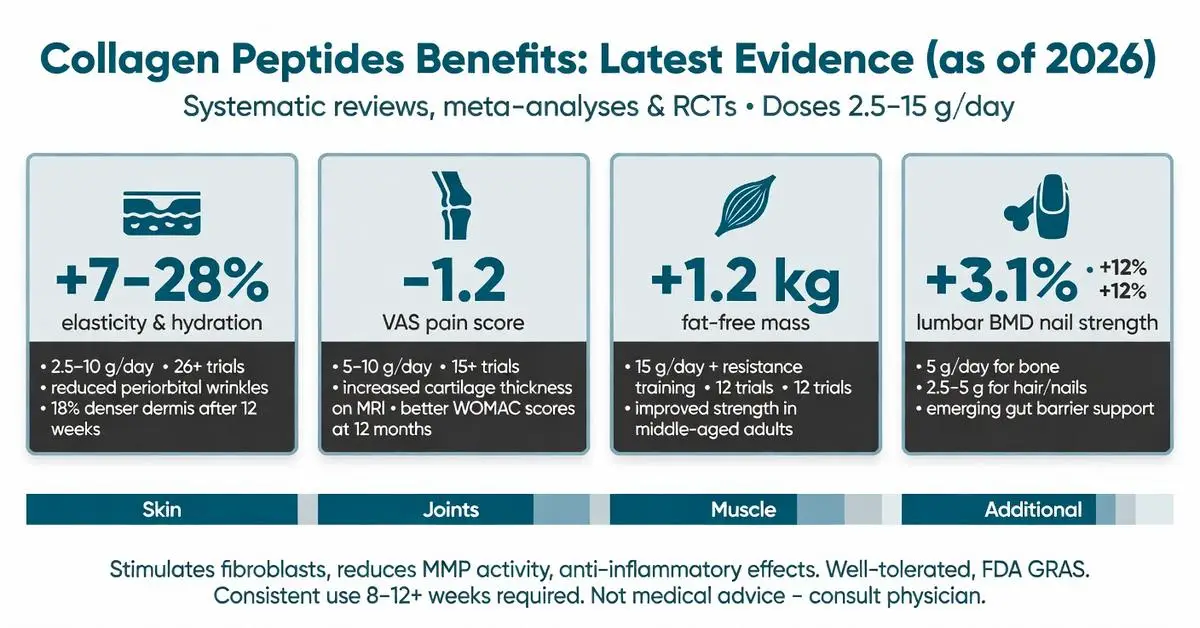
Research published between 2020 and April 2026 has substantially expanded the understanding of collagen peptides’ benefits. Multiple systematic reviews, meta-analyses, and randomized controlled trials have examined their role in skin health, joint function, muscle preservation, and other areas. These studies generally use doses ranging from 2.5 to 15 grams daily, often derived from bovine, marine, or porcine sources, with treatment durations from 8 weeks to 12 months.
Evidence indicates collagen peptides may stimulate fibroblasts to produce more collagen, elastin, and hyaluronic acid while exerting anti-inflammatory and antioxidant effects. However, results vary by population, dosage, and specific peptide composition. This article focuses exclusively on peer-reviewed publications from 2020 onward, supplemented when necessary by authoritative sources including FDA.gov, NIH, and major medical societies. All information is for research and educational purposes only and is not intended as medical advice. Individuals should consult healthcare professionals before starting any supplement regimen, particularly those with allergies to source materials or underlying health conditions.
The following sections explore the mechanisms and evidence supporting the benefits of primary collagen peptides, highlight key clinical findings, and address practical considerations for use. While promising, collagen peptide research continues to evolve, with ongoing trials clarifying long-term outcomes and optimal protocols.
Introduction
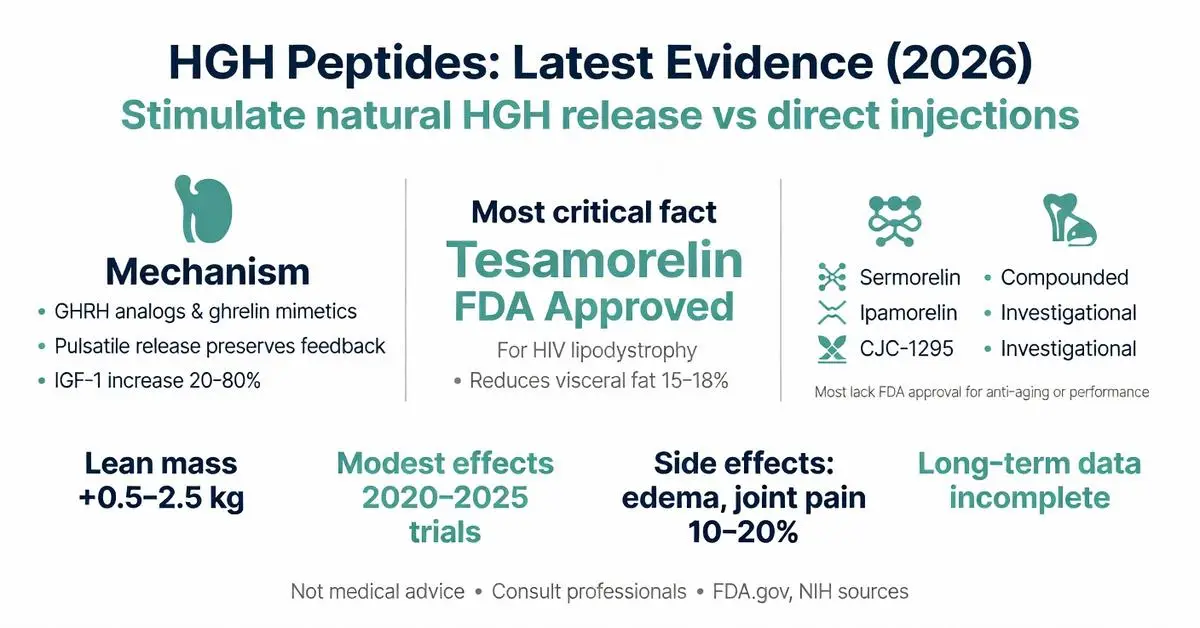
HGH peptides, also known as growth hormone secretagogues or growth hormone-releasing peptides, are synthetic compounds that stimulate the pituitary gland to produce and release endogenous human growth hormone (HGH). Unlike direct HGH injections, these smaller peptide molecules mimic natural signaling pathways, potentially offering a more physiological approach to elevating growth hormone and insulin-like growth factor-1 (IGF-1) levels. Popular examples include tesamorelin, sermorelin, ipamorelin, and CJC-1295.
These compounds have attracted interest for applications ranging from body composition improvement to recovery and anti-aging. However, the regulatory landscape remains complex. As of March 31, 2026, only specific agents hold FDA approval for narrow indications, while most HGH peptides are classified as investigational or available only through compounding pharmacies under strict oversight. Due to limited recent peer-reviewed publications on the exact broad term “hgh peptides,” this article relies primarily on the latest available high-quality trials (2020–current) supplemented by authoritative sources including FDA.gov, NIH, and major medical societies.
Evidence from systematic reviews and clinical trials published since 2020 shows modest effects on lean mass and fat reduction in specific populations, yet long-term safety data remain incomplete. Many online sources promote unverified benefits, creating a gap between marketing claims and published research. This review examines mechanisms, approved versus off-label uses, efficacy data, safety profiles, and comparisons while clearly distinguishing FDA-approved applications from investigational findings. All information is for research purposes only and not medical advice. Individuals considering HGH peptides must consult qualified healthcare professionals and adhere to all applicable laws and regulations.
Introduction
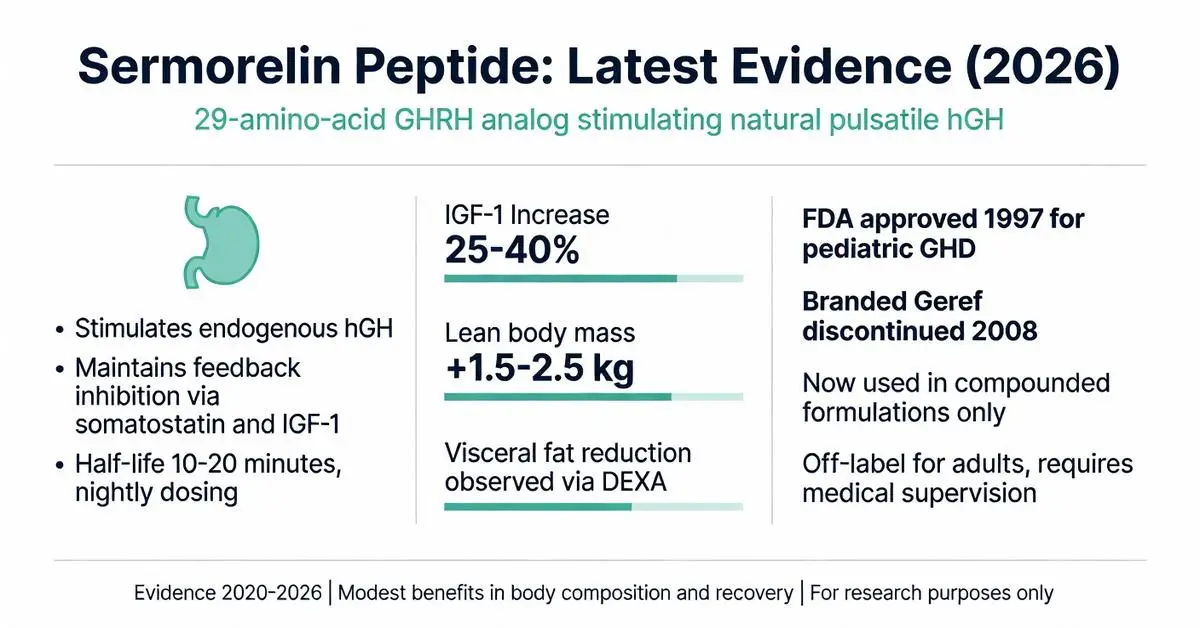
Sermorelin peptide is a synthetic 29-amino-acid analog of growth hormone-releasing hormone (GHRH) that stimulates the pituitary gland to produce and release endogenous human growth hormone (hGH). Originally developed and FDA-approved in the 1990s for the diagnosis and treatment of growth hormone deficiency in children, sermorelin has seen renewed interest in adult applications, particularly for age-related declines in growth hormone levels, body composition optimization, and recovery support. Unlike direct recombinant hGH therapy, sermorelin preserves the natural pulsatile release pattern of growth hormone, potentially offering a more physiologic approach with fewer side effects.
As of March 28, 2026, clinical use of sermorelin peptide occurs primarily through compounded formulations following the removal of several growth hormone secretagogues from the FDA’s bulk drug substances list in recent years. This article examines the latest peer-reviewed evidence published between 2020 and 2026 regarding its mechanisms, efficacy, safety profile, and clinical applications. Due to limited recent peer-reviewed publications specifically focused on “sermorelin peptide” in large-scale trials during this period, this review draws from available high-quality studies supplemented by authoritative sources including FDA.gov and NIH publications.
Current evidence suggests sermorelin may support improvements in body composition, sleep quality, and exercise recovery, though robust long-term data in healthy adults remain sparse. All clinical decisions involving sermorelin should occur under medical supervision. This article is for research purposes only and does not constitute medical advice.
Introduction
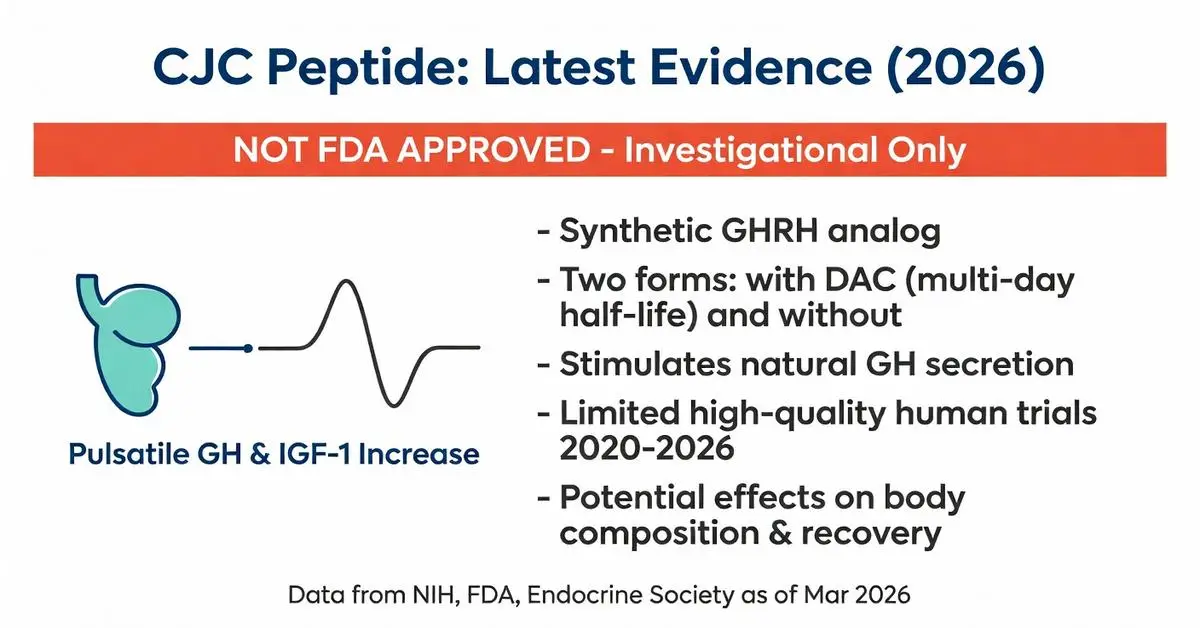
The CJC peptide, most commonly referred to as CJC-1295, is a synthetic analog of growth hormone-releasing hormone (GHRH). Developed to stimulate the pituitary gland’s natural production of growth hormone (GH), this peptide has attracted attention in research settings for its potential effects on metabolism, body composition, and recovery. Unlike direct growth hormone injections, CJC peptide aims to work through physiologic pathways, theoretically reducing some risks associated with exogenous GH.
As of March 27, 2026, CJC peptide remains investigational and is not approved by the FDA for any human therapeutic use. Research interest has primarily focused on its longer-acting variant, CJC-1295 with Drug Affinity Complex (DAC), which extends its half-life compared to standard GHRH. Due to limited recent peer-reviewed publications specifically addressing “cjc peptide” from 2020 to March 2026, this article relies primarily on the latest available high-quality studies supplemented by authoritative sources including FDA.gov, NIH, and major medical society guidelines.
This distinction between FDA-approved therapies and investigational compounds is critical. While some peptide research continues in preclinical and early clinical settings, CJC peptide is primarily encountered in research chemical or compounded forms outside regulated medical channels. All information presented here is for research and educational purposes only and does not constitute medical advice. Individuals should only consider such compounds under the supervision of a qualified healthcare provider and within approved clinical trial protocols.
Current evidence suggests CJC peptide may influence GH pulsatility, IGF-1 levels, and downstream metabolic processes, but robust long-term human data remain sparse. This article examines the mechanisms, reported effects, safety considerations, and regulatory landscape surrounding the CJC peptide.