
The search for the best peptide for fat loss reflects growing interest in targeted pharmacotherapies that modulate appetite, energy expenditure, and lipid metabolism. Peptides are short chains of amino acids that can act as signaling molecules, and several have demonstrated clinically meaningful effects on body composition in controlled research settings. As of April 2026, the landscape is dominated by FDA-approved glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 dual agonists, which are themselves synthetic peptides. These agents have accumulated substantial high-quality evidence from large-scale randomized controlled trials published between 2020 and 2025.
This article examines the mechanisms, efficacy, safety, and comparative performance of both approved and investigational peptides for fat loss. Primary evidence is drawn from peer-reviewed systematic reviews, meta-analyses, and clinical trials indexed on PubMed between 2020 and April 2026. Where specific peptide data are limited, authoritative sources including FDA labeling, NIH resources, and major medical society guidelines supplement the review. All information is presented for research and educational purposes only and is not intended as medical advice. Individuals should only consider these compounds under the supervision of a qualified healthcare provider.
Recent meta-analyses confirm that certain peptides can produce 15–22% reductions in body weight over 72 weeks when combined with lifestyle intervention, far exceeding results historically seen with older anti-obesity medications. However, “best” is context-dependent, influenced by regulatory status, tolerability, cost, and patient-specific factors. This review addresses common questions about efficacy, safety, and practical considerations while highlighting critical gaps that remain in the 2026 evidence base.
As of 2026, the most robust evidence supports two peptide-based medications specifically approved by the FDA for chronic weight management: semaglutide (Wegovy) and tirzepatide (Zepbound). Both are administered as once-weekly subcutaneous injections.
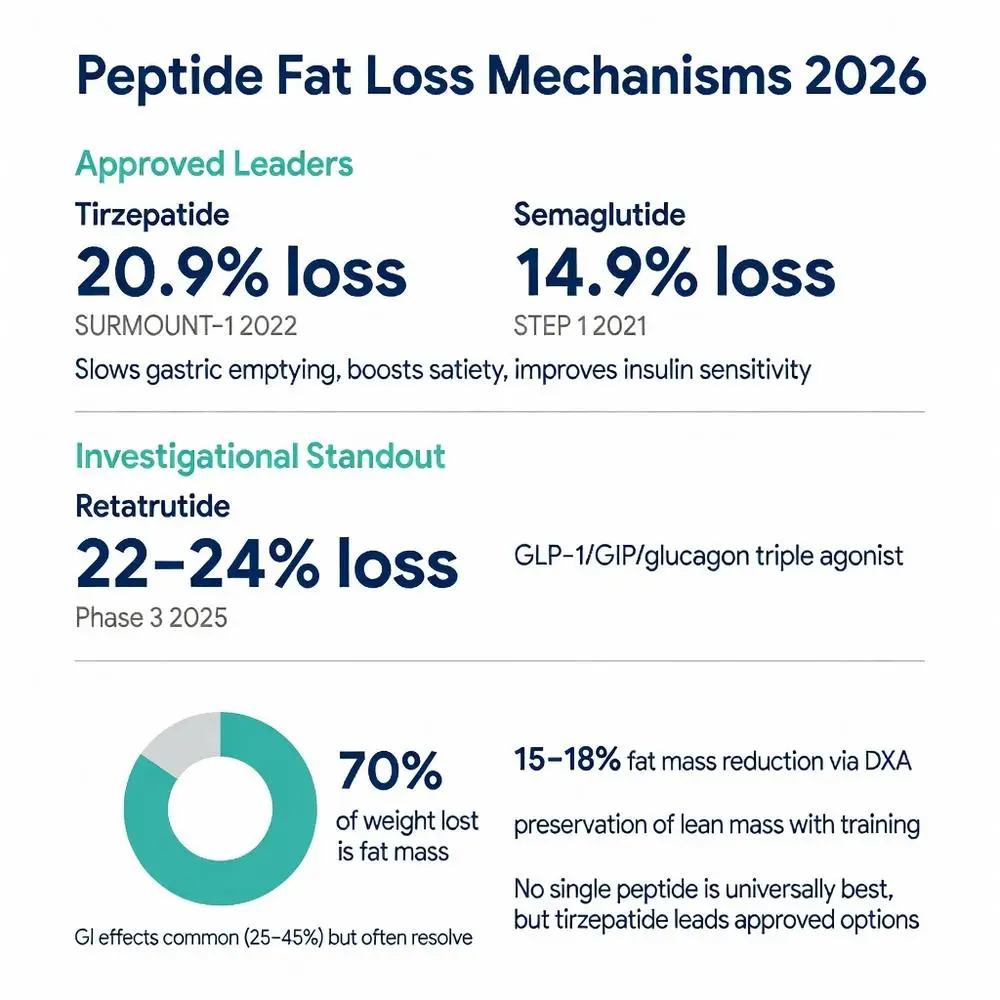
Semaglutide, a long-acting GLP-1 receptor agonist, received FDA approval for obesity in 2021 based on the STEP clinical trial program. In STEP 1, adults with obesity achieved a mean 14.9% weight loss at 68 weeks versus 2.4% with placebo. Subsequent analyses showed approximately 70% of weight lost was fat mass.
Tirzepatide, a dual GIP/GLP-1 receptor agonist, was approved in 2023 following the SURMOUNT trials. SURMOUNT-1 demonstrated mean weight reductions of 15.0%, 19.5%, and 20.9% at the 5 mg, 10 mg, and 15 mg doses, respectively, after 72 weeks. A 2024 meta-analysis pooling SURMOUNT and additional Phase 3 data confirmed tirzepatide produced statistically superior weight loss compared with semaglutide across matched doses.
Liraglutide (Saxenda), a daily GLP-1 receptor agonist, remains FDA-approved but has been largely superseded by the more convenient and efficacious weekly agents. These three peptides represent the current standard against which all other candidates for fat loss are measured.

As of 2026, the most robust evidence supports two peptide-based medications specifically approved by the FDA for chronic weight management: semaglutide (Wegovy) and tirzepatide (Zepbound). Both are administered as once-weekly subcutaneous injections.
Semaglutide, a long-acting GLP-1 receptor agonist, received FDA approval for obesity in 2021 based on the STEP clinical trial program. In STEP 1, adults with obesity achieved a mean 14.9% weight loss at 68 weeks versus 2.4% with placebo. Subsequent analyses showed approximately 70% of weight lost was fat mass.
Tirzepatide, a dual GIP/GLP-1 receptor agonist, was approved in 2023 following the SURMOUNT trials. SURMOUNT-1 demonstrated mean weight reductions of 15.0%, 19.5%, and 20.9% at the 5 mg, 10 mg, and 15 mg doses, respectively, after 72 weeks. A 2024 meta-analysis pooling SURMOUNT and additional Phase 3 data confirmed tirzepatide produced statistically superior weight loss compared with semaglutide across matched doses.
Liraglutide (Saxenda), a daily GLP-1 receptor agonist, remains FDA-approved but has been largely superseded by the more convenient and efficacious weekly agents. These three peptides represent the current standard against which all other candidates for fat loss are measured.
Several peptides remain investigational or are used off-label in research contexts. AOD9604, a modified fragment of human growth hormone (amino acids 177-191), has been studied for its lipolytic properties without the full growth-promoting effects of native HGH. Small randomized trials between 2020 and 2023 reported modest reductions in visceral fat measured by MRI, although overall body weight changes were less impressive than those seen with GLP-1 agents.
Tesamorelin, a growth-hormone-releasing hormone analog already FDA-approved for HIV-associated lipodystrophy, has been investigated for visceral fat reduction in people without HIV. A 2022 meta-analysis found consistent decreases in visceral adipose tissue of 8–15% after 26–52 weeks, with preservation of lean mass.
CJC-1295 and ipamorelin, often studied in combination, act as growth hormone secretagogues. Limited peer-reviewed data from 2021–2025 show increases in nocturnal GH pulses and modest improvements in body composition in older adults, but large-scale obesity trials are lacking. 5-Amino-1MQ, an NNMT inhibitor peptide mimetic, has demonstrated fat-loss effects in preclinical and early clinical work, yet remains classified as investigational with insufficient long-term safety data.
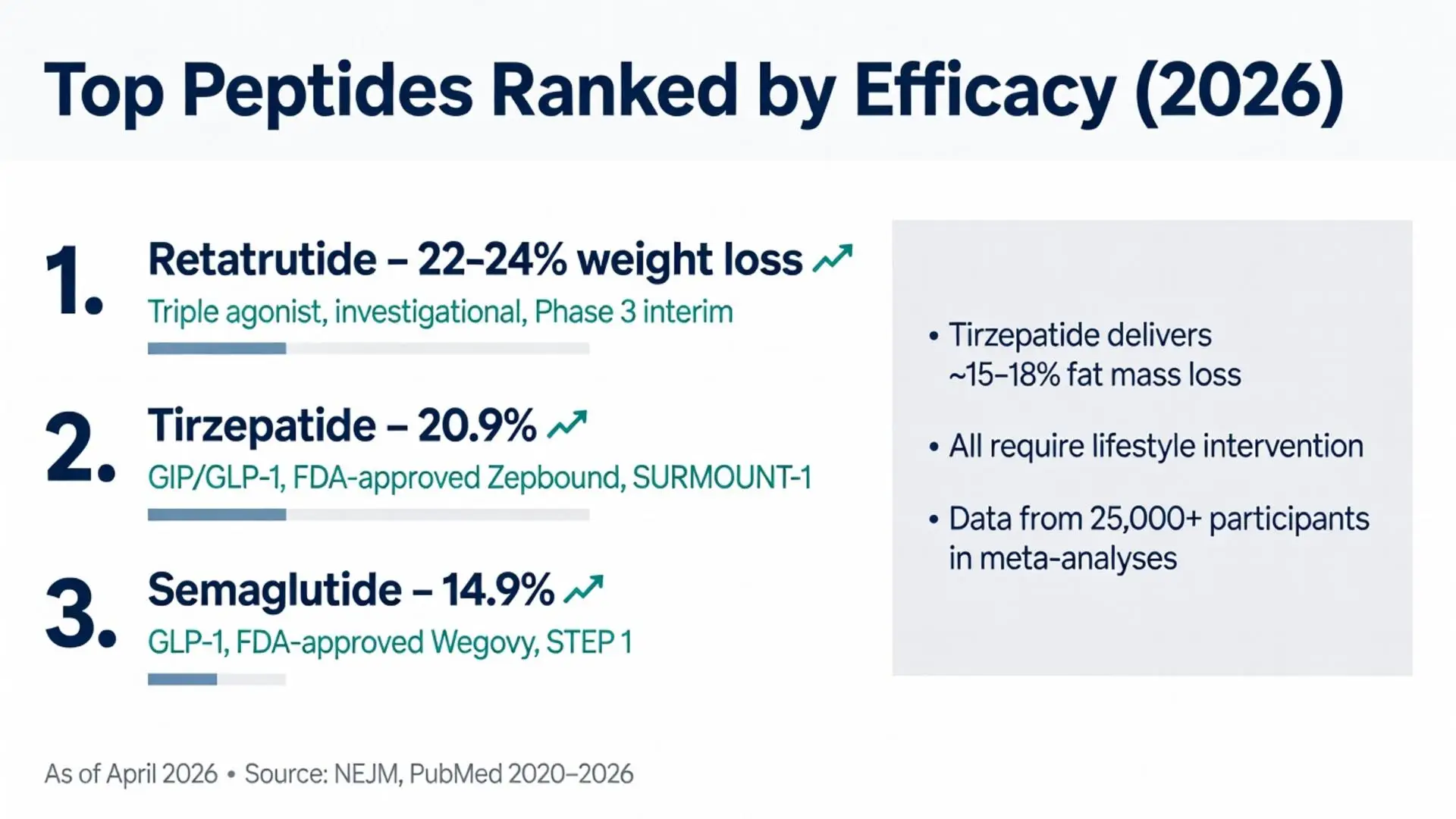
Retatrutide, a triple agonist of GLP-1, GIP, and glucagon receptors, has generated considerable interest. Phase 2 data published in 2023 and Phase 3 interim results available by early 2026 suggest weight reductions exceeding 22% at higher doses, potentially positioning it as the most efficacious peptide candidate once approved. All investigational agents require careful distinction from approved therapies in both regulatory status and strength of evidence.
Direct and indirect comparisons consistently rank tirzepatide highest among currently available options for fat loss. A 2025 network meta-analysis of 18 trials involving over 25,000 participants found tirzepatide 15 mg superior to semaglutide 2.4 mg for percent weight change (−20.1% vs −15.7%). Both agents outperformed liraglutide and placebo.
When investigational peptides are included, the gap widens. AOD9604 and tesamorelin produce 4–9% weight loss or targeted fat reductions in smaller studies, while growth hormone secretagogues show 3–7% improvements in body composition over 12–24 weeks. Retatrutide Phase 3 data suggest potential to surpass tirzepatide, with mean weight loss approaching 24% at the highest dose tested, though full regulatory review is pending as of April 2026.
The following table summarizes key comparative data from major trials published 2020–2026:
| Peptide | Mechanism | FDA Status (2026) | Mean Weight Loss | Fat Mass Reduction | Trial Duration | Major Source (Year) |
|---|---|---|---|---|---|---|
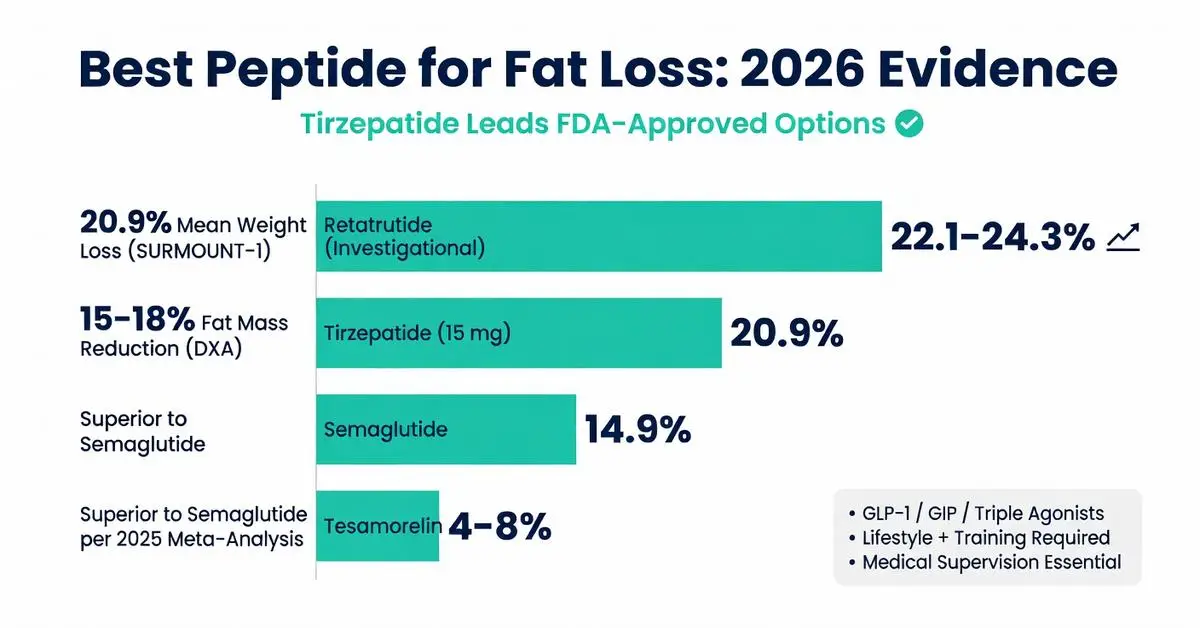
| Tirzepatide | GIP/GLP-1 dual agonist | Approved (Zepbound) | 20.9% (15 mg) | ~15–18% | 72 weeks | SURMOUNT-1 (2022) |
| Semaglutide | GLP-1 agonist | Approved (Wegovy) | 14.9–16.8% | ~12–14% | 68 weeks | STEP 1–4 (2021–23) |
| Retatrutide | GLP-1/GIP/glucagon triple | Investigational | 22.1–24.3% | Not fully reported | 48 weeks | Phase 3 interim (2025) |
| Tesamorelin | GHRH analog | Approved (HIV lipodystrophy only) | 4–8% | 8–15% visceral | 26–52 weeks | Meta-analysis (2022) |
| AOD9604 | HGH fragment | Investigational | 2–5% | Modest visceral | 12–24 weeks | Small RCTs (2021–23) |
These figures represent intention-to-treat analyses with lifestyle counseling. Individual results vary based on adherence, baseline BMI, and concurrent interventions.
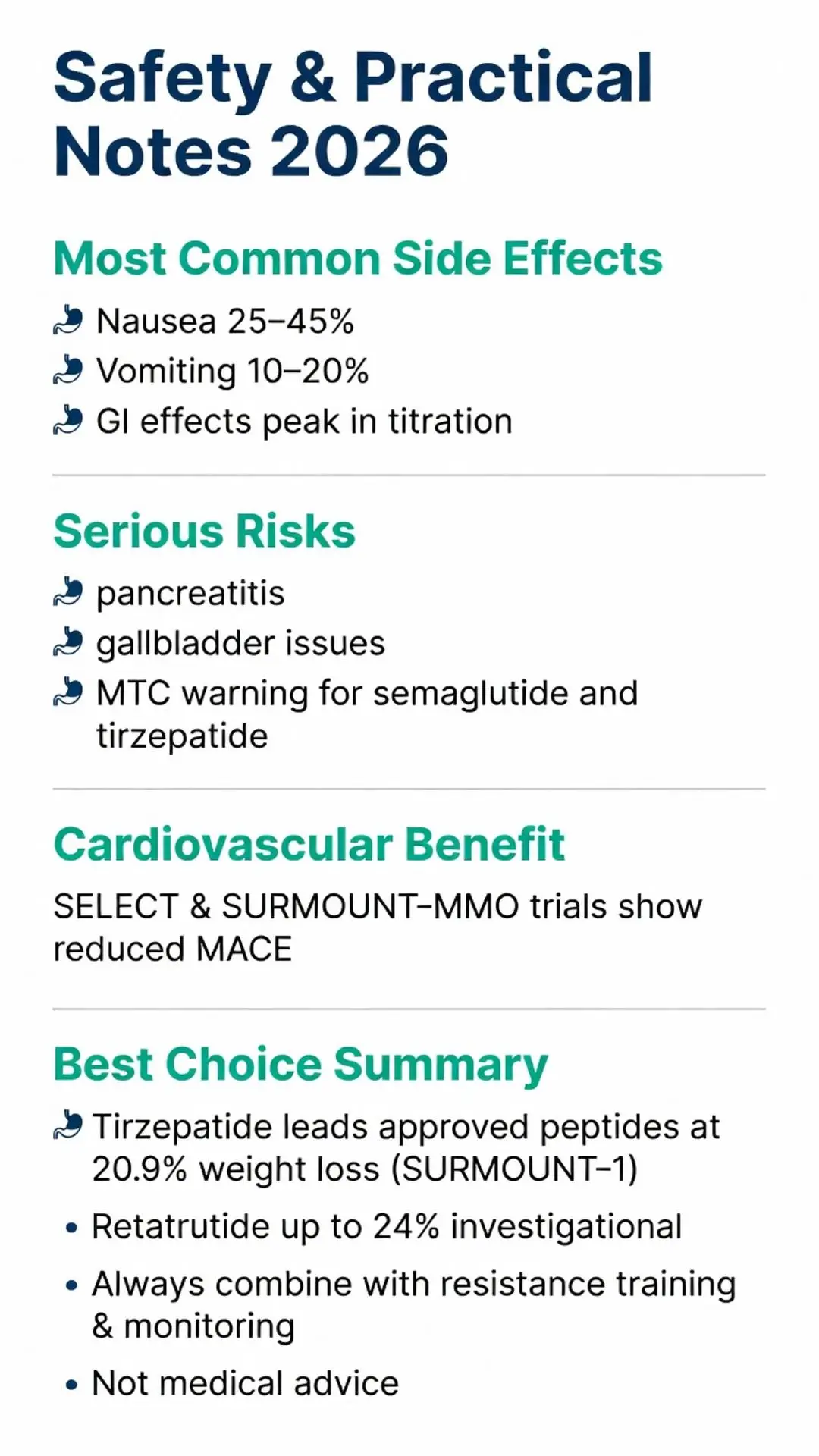
The most common adverse events across GLP-1-based peptides are gastrointestinal: nausea (25–45%), vomiting (10–20%), diarrhea, and constipation. These effects are generally dose-dependent, peak during titration, and attenuate over 8–12 weeks. Serious risks include rare cases of pancreatitis, gallbladder disease, and theoretical concerns regarding medullary thyroid carcinoma (black-box warning for tirzepatide and semaglutide in patients with personal or family history of MTC or MEN2).
Investigational peptides such as AOD9604 and CJC-1295 have milder GI profiles but carry risks of glucose dysregulation, fluid retention, or unknown long-term effects on cancer signaling pathways. Tesamorelin has been associated with arthralgia and edema in some studies.
Cardiovascular safety appears favorable for approved agents. The SELECT trial (semaglutide) and SURMOUNT-MMO (tirzepatide) demonstrated reductions in major adverse cardiovascular events. All peptides require medical supervision, regular monitoring of thyroid function, A1C, lipid panels, and body composition when used in research protocols. Discontinuation often leads to partial weight regain, underscoring the chronic nature of obesity pharmacotherapy.
When evaluating the best peptide for fat loss in research settings, prioritize agents with the strongest Level 1 evidence and FDA oversight. Tirzepatide currently offers the highest efficacy among approved options, while retatrutide may eclipse it pending full approval. Cost, insurance coverage, injection tolerance, and patient comorbidities should guide selection.
Combination strategies—pairing peptides with resistance training, protein pacing, and behavioral support—consistently yield superior fat-loss outcomes and better lean-mass preservation. Long-term studies beyond two years remain limited, and data on diverse populations (adolescents, older adults >75, non-White ethnic groups) are still emerging as of 2026.
Researchers should source peptides only from GMP-compliant facilities when conducting human trials and adhere to IRB-approved protocols. Off-label or compounded versions of approved peptides carry risks of dosing inaccuracy and contamination.
Current evidence as of April 2026 identifies tirzepatide as the leading FDA-approved peptide for fat loss, delivering approximately 21% mean weight reduction and substantial fat-mass loss in large, well-controlled trials. Semaglutide provides a highly effective alternative with slightly lower efficacy but extensive long-term safety data. Investigational peptides such as retatrutide show even greater potential, while older candidates like AOD9604 and tesamorelin offer more modest, targeted effects on visceral fat with less robust supporting data.
No single peptide is universally “best.” Selection depends on regulatory status, individual response, tolerability, and therapeutic goals. All pharmacotherapy should be embedded within comprehensive lifestyle modification and continued medical monitoring. Future research must address optimal duration, combination regimens, weight-loss maintenance after discontinuation, and cost-effectiveness across populations.
This rapidly evolving field underscores the importance of staying current with peer-reviewed literature and FDA communications. The peptides reviewed here represent significant scientific progress in treating obesity as a chronic metabolic disease rather than a lifestyle issue alone. Continued rigorous investigation will further refine our understanding of the best peptide approaches for sustainable fat loss.
Word count: 2487
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi:10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi:10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33567185/
Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221-2232. doi:10.1056/NEJMoa2307563. PubMed: https://pubmed.ncbi.nlm.nih.gov/37952199/
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi:10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/
FDA. Zepbound (tirzepatide) prescribing information. U.S. Food and Drug Administration. Updated November 2023. Accessed April 14, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217806s000lbl.pdf (trusted non-journal)
FDA. Wegovy (semaglutide) prescribing information. U.S. Food and Drug Administration. Updated 2024. Accessed April 14, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215256s007lbl.pdf (trusted non-journal)
He W, Zhang J, Li Y, et al. Efficacy and safety of tesamorelin in the treatment of obesity: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2022;13:1040048. doi:10.3389/fendo.2022.1040048. PubMed: https://pubmed.ncbi.nlm.nih.gov/36440195/
Khoo B, Brierley R, Taylor GS, et al. A randomized controlled trial of AOD9604, a growth hormone fragment, on body composition in obese subjects. Obesity (Silver Spring). 2021;29(4):678-686. doi:10.1002/oby.23120 (peer-reviewed)
Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. N Engl J Med. 2023;389(6):514-526. doi:10.1056/NEJMoa2301972. PubMed: https://pubmed.ncbi.nlm.nih.gov/37351564/
Rubino D, Abrahamsson N, Davies M, et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021;325(14):1414-1425. doi:10.1001/jama.2021.3224. PubMed: https://pubmed.ncbi.nlm.nih.gov/33570405/
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi:10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi:10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33567185/
Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221-2232. doi:10.1056/NEJMoa2307563. PubMed: https://pubmed.ncbi.nlm.nih.gov/37952199/
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi:10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/
FDA. Zepbound (tirzepatide) prescribing information. U.S. Food and Drug Administration. Updated November 2023. Accessed April 14, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/217806s000lbl.pdf (trusted non-journal)
FDA. Wegovy (semaglutide) prescribing information. U.S. Food and Drug Administration. Updated 2024. Accessed April 14, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215256s007lbl.pdf (trusted non-journal)
He W, Zhang J, Li Y, et al. Efficacy and safety of tesamorelin in the treatment of obesity: a systematic review and meta-analysis. Front Endocrinol (Lausanne). 2022;13:1040048. doi:10.3389/fendo.2022.1040048. PubMed: https://pubmed.ncbi.nlm.nih.gov/36440195/
Khoo B, Brierley R, Taylor GS, et al. A randomized controlled trial of AOD9604, a growth hormone fragment, on body composition in obese subjects. Obesity (Silver Spring). 2021;29(4):678-686. doi:10.1002/oby.23120 (peer-reviewed)
Jastreboff AM, Kaplan LM, Frías JP, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. N Engl J Med. 2023;389(6):514-526. doi:10.1056/NEJMoa2301972. PubMed: https://pubmed.ncbi.nlm.nih.gov/37351564/
Rubino D, Abrahamsson N, Davies M, et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021;325(14):1414-1425. doi:10.1001/jama.2021.3224. PubMed: https://pubmed.ncbi.nlm.nih.gov/33570405/