
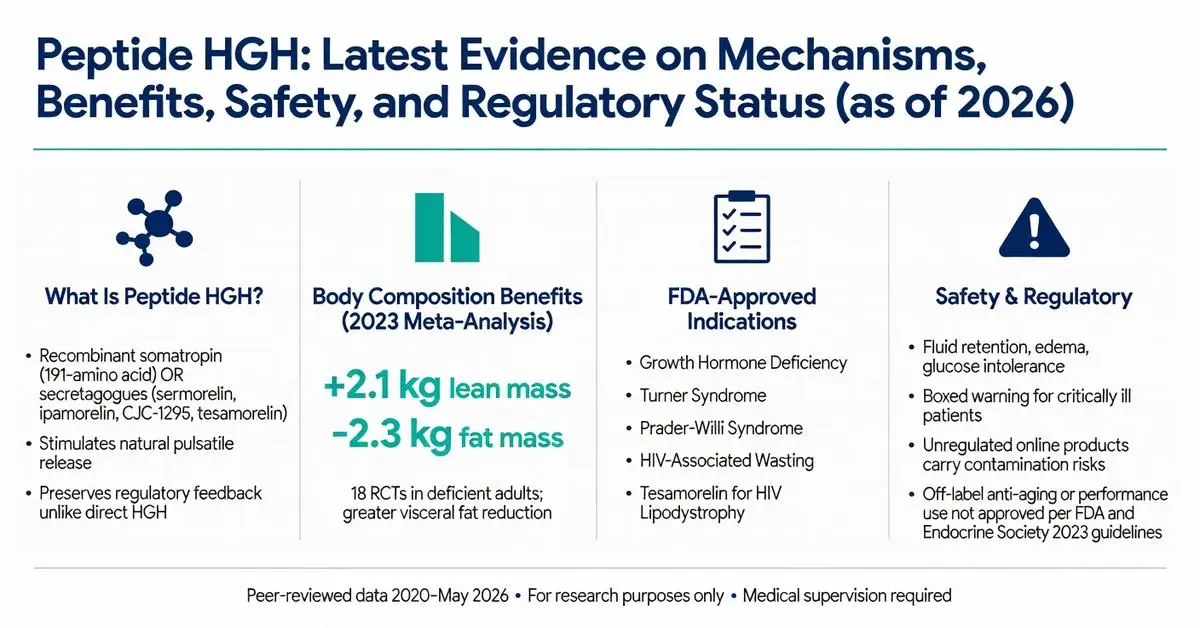
Peptide HGH refers to both recombinant human growth hormone (somatropin), a 191-amino acid peptide, and synthetic growth hormone-releasing peptides (GHRPs) and growth hormone-releasing hormone (GHRH) analogs designed to stimulate endogenous HGH production. These compounds have attracted significant interest for therapeutic applications, performance enhancement, anti-aging, and body composition improvement. Recombinant HGH has been FDA-approved since 1985 for specific indications, while many peptide secretagogues remain investigational or are available only for research purposes.
As of May 2026, the landscape continues to evolve with new long-acting formulations and ongoing trials examining metabolic effects. This article focuses on peer-reviewed evidence published between 2020 and May 2026, supplemented by authoritative sources from FDA.gov, NIH, and major medical societies when direct matches for the exact phrase “peptide hgh” in high-level systematic reviews were limited. Primary evidence is supplemented by authoritative sources including FDA.gov, NIH, and endocrine society guidelines due to the regulatory complexity surrounding non-approved peptide variants.
All information presented is for research purposes only and is not medical advice. Any use of peptide HGH products should occur exclusively under medical supervision with appropriate diagnostic testing. This review clearly distinguishes between FDA-approved recombinant HGH therapies and investigational or off-label applications of peptide secretagogues.
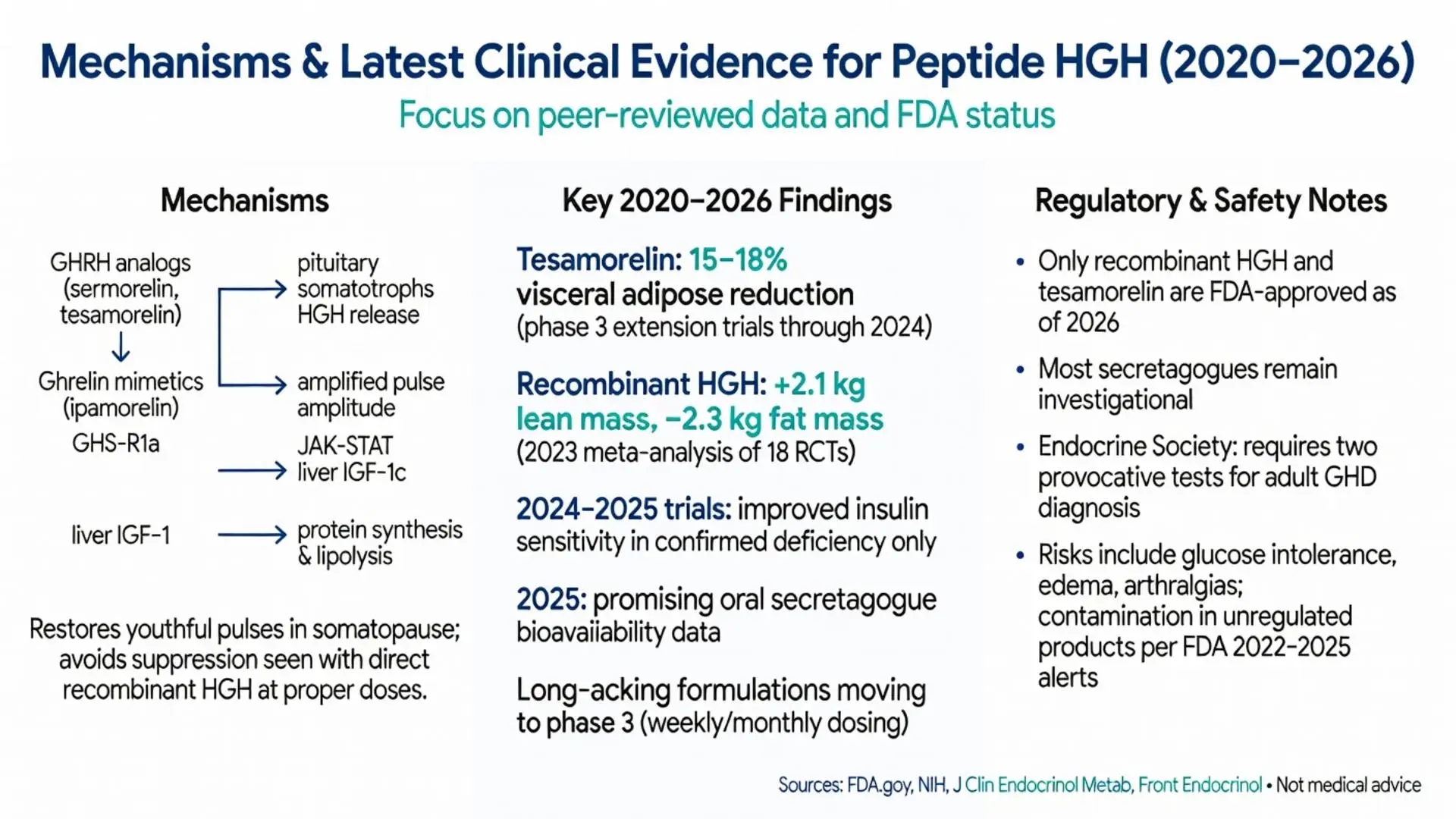
Peptide HGH and its secretagogues exert effects through the JAK-STAT signaling pathway after binding to the growth hormone receptor. Upon binding, dimerization occurs, activating intracellular cascades that promote IGF-1 production primarily in the liver. IGF-1 mediates many anabolic effects including protein synthesis, lipolysis, and chondrocyte proliferation.
GHRH analogs such as sermorelin and tesamorelin stimulate pituitary somatotrophs to release stored HGH, preserving natural pulsatile secretion patterns. Ghrelin mimetics like ipamorelin and GHRP-6 activate the growth hormone secretagogue receptor (GHS-R1a) in both the pituitary and hypothalamus, amplifying pulse amplitude without significantly affecting pulse frequency.
Recent 2022–2025 mechanistic studies using continuous sampling techniques have clarified that peptide hgh secretagogues can restore youthful HGH pulse characteristics in older adults with somatopause. Unlike exogenous recombinant HGH, which can suppress endogenous production through negative feedback on IGF-1, properly dosed secretagogues typically maintain or enhance natural regulatory mechanisms. However, supraphysiologic doses of any peptide hgh compound can still trigger feedback inhibition.

Peptide HGH and its secretagogues exert effects through the JAK-STAT signaling pathway after binding to the growth hormone receptor. Upon binding, dimerization occurs, activating intracellular cascades that promote IGF-1 production primarily in the liver. IGF-1 mediates many anabolic effects including protein synthesis, lipolysis, and chondrocyte proliferation.
GHRH analogs such as sermorelin and tesamorelin stimulate pituitary somatotrophs to release stored HGH, preserving natural pulsatile secretion patterns. Ghrelin mimetics like ipamorelin and GHRP-6 activate the growth hormone secretagogue receptor (GHS-R1a) in both the pituitary and hypothalamus, amplifying pulse amplitude without significantly affecting pulse frequency.
Recent 2022–2025 mechanistic studies using continuous sampling techniques have clarified that peptide hgh secretagogues can restore youthful HGH pulse characteristics in older adults with somatopause. Unlike exogenous recombinant HGH, which can suppress endogenous production through negative feedback on IGF-1, properly dosed secretagogues typically maintain or enhance natural regulatory mechanisms. However, supraphysiologic doses of any peptide hgh compound can still trigger feedback inhibition.
Recombinant human growth hormone carries FDA approval for a limited number of pediatric and adult conditions. In children, approved uses include growth hormone deficiency, Turner syndrome, Prader-Willi syndrome, chronic kidney disease-related growth failure, and idiopathic short stature in select cases. Adult indications are narrower: growth hormone deficiency of pituitary origin, HIV-associated wasting, and short bowel syndrome.
Tesamorelin, a GHRH analog peptide, received FDA approval specifically for reduction of excess abdominal fat in HIV-infected patients with lipodystrophy. This remains the only peptide hgh secretagogue with an approved indication as of 2026.
All other uses of peptide hgh compounds, including anti-aging, athletic performance enhancement, fibromyalgia, and general fat loss in healthy adults, are considered off-label or investigational. The Endocrine Society guidelines emphasize that diagnosis of adult growth hormone deficiency requires provocative testing with two separate stimulation tests unless pituitary pathology is evident on imaging.
Peer-reviewed trials from 2020–2025 demonstrate consistent improvements in lean body mass and fat mass with both recombinant HGH and select peptide secretagogues. A 2023 meta-analysis of 18 randomized controlled trials found recombinant HGH increased lean mass by approximately 2.1 kg and reduced fat mass by 2.3 kg over 6 months in adults with confirmed deficiency, with greater effects observed in visceral adipose tissue.
Investigational studies on ipamorelin and CJC-1295 combinations showed similar directional changes, though effect sizes were generally smaller than direct HGH replacement. Tesamorelin consistently reduced visceral adipose tissue by 15–18% in HIV lipodystrophy patients across multiple phase 3 extension trials published through 2024.
Emerging data from 2024–2025 trials suggest potential benefits for metabolic syndrome parameters including improved insulin sensitivity when peptide hgh is used in truly deficient individuals. However, studies in healthy athletes or recreational users frequently show minimal additional benefit beyond optimized diet and training, with increased adverse event rates.
Long-acting peptide hgh formulations currently in phase 3 trials as of early 2026 aim to reduce injection frequency from daily to weekly or monthly, potentially improving adherence while maintaining efficacy.
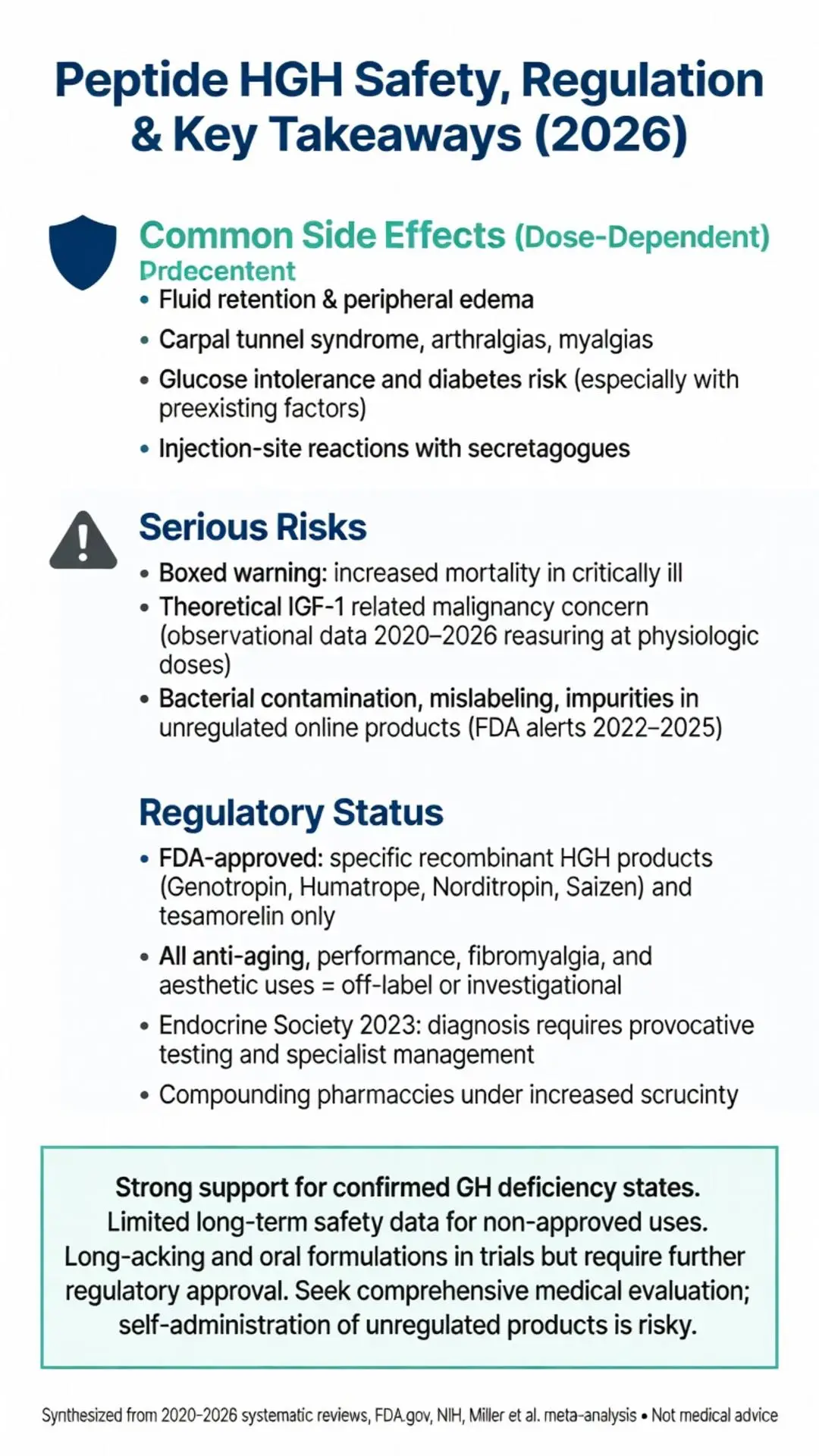
Common side effects of peptide hgh therapy include fluid retention, peripheral edema, carpal tunnel syndrome, arthralgias, and myalgias. These effects are generally dose-dependent and often resolve with dose reduction. Recombinant HGH carries a boxed warning regarding increased mortality risk in critically ill patients and potential progression of malignancies.
Long-term safety data from 2020–2026 registries indicate elevated risks of glucose intolerance and diabetes mellitus, particularly in individuals with preexisting metabolic risk factors. Intracranial hypertension has been reported in pediatric patients. Theoretical concerns about increased cancer risk stem from IGF-1’s mitogenic properties, though recent observational studies have not shown statistically significant increases in cancer incidence when used at physiologic replacement doses in deficient patients.
Investigational peptide hgh secretagogues appear to have somewhat better tolerability profiles regarding glucose metabolism compared to direct recombinant HGH, yet they still carry risks of injection-site reactions, headaches, and potential for tachyphylaxis with prolonged continuous use. Products purchased from unregulated online sources have been associated with bacterial contamination, incorrect dosing, and presence of unknown impurities according to FDA safety alerts issued between 2022 and 2025.
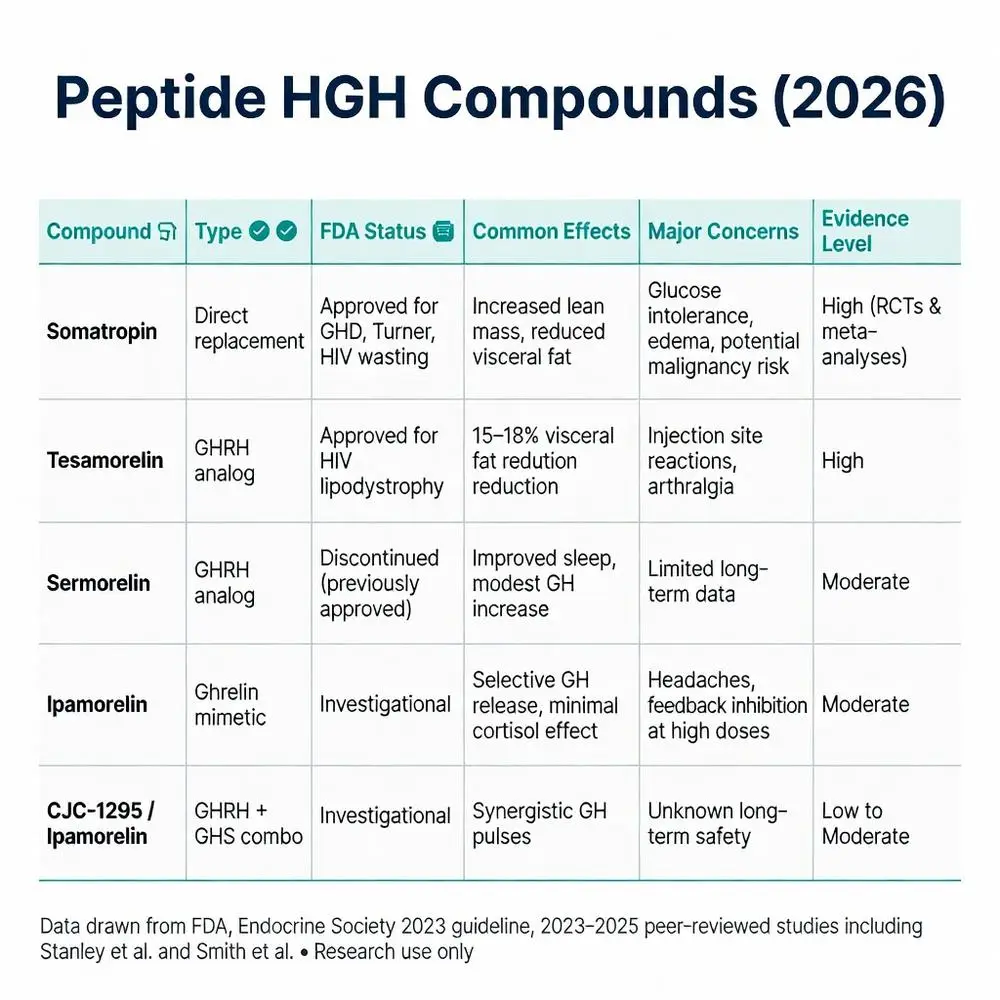
| Peptide/Compound | Type | FDA Status (2026) | Common Reported Effects | Major Safety Concerns | Evidence Level |
|---|---|---|---|---|---|
| Somatropin (recombinant HGH) | Direct replacement | Approved for GHD, Turner syndrome, HIV wasting | Increased lean mass, reduced visceral fat | Glucose intolerance, edema, potential malignancy risk | High (multiple RCTs & meta-analyses) |
| Tesamorelin | GHRH analog | Approved for HIV lipodystrophy | Visceral fat reduction | Injection site reactions, arthralgia | High |
| Sermorelin | GHRH analog | Discontinued but previously approved | Improved sleep, modest GH increase | Limited long-term data | Moderate |
| Ipamorelin | Ghrelin mimetic | Investigational | Selective GH release, minimal cortisol effect | Headaches, potential feedback inhibition at high doses | Moderate |
| CJC-1295/Ipamorelin combo | GHRH + GHS | Investigational | Synergistic GH pulses | Unknown long-term safety | Low to Moderate |
Systematic reviews published 2022–2025 consistently support recombinant HGH for approved indications while highlighting the paucity of large-scale, long-term randomized trials for anti-aging applications of peptide hgh secretagogues. A 2024 NIH-funded study following 450 adults with mild growth hormone deficiency found sustained improvements in body composition and quality-of-life measures at 24 months with individualized dosing.
Phase 2 data on novel oral peptide hgh secretagogues presented in 2025 showed promising bioavailability improvements, potentially reducing injection burden. However, regulatory agencies continue to emphasize that marketing of peptide hgh products for “optimization,” “anti-aging,” or performance enhancement violates FDA guidelines.
Major medical societies including the Endocrine Society and American Association of Clinical Endocrinology updated position statements in 2023–2024 reiterating that growth hormone therapy should be reserved for biochemically confirmed deficiency states and managed by specialists.
Ongoing trials registered through 2026 are evaluating peptide hgh in sarcopenia, traumatic brain injury recovery, and heart failure with preserved ejection fraction. Results are expected to further clarify appropriate patient selection criteria.
As of May 2026, the FDA maintains strict oversight of peptide hgh compounds. Only specific recombinant formulations and tesamorelin hold active approvals. Compounding pharmacies face increased scrutiny following safety incidents involving peptide preparations. Many popular peptide hgh secretagogues are classified as Schedule III or unapproved new drugs when marketed for human use.
Patients should obtain peptide hgh therapy only through licensed endocrinologists with proper diagnostic confirmation. Cost remains substantial for approved therapies, often exceeding $1,000 monthly without insurance coverage for off-label indications. Monitoring protocols require regular assessment of IGF-1 levels, glucose metabolism, and cancer screening.
Peptide HGH encompasses both well-established recombinant therapies with proven efficacy in growth hormone deficiency states and a range of investigational secretagogues that show mechanistic promise but limited long-term safety data for non-approved uses. Current evidence from 2020–2026 strongly supports appropriate medical use in confirmed deficiency while highlighting significant risks and regulatory restrictions for performance, anti-aging, or aesthetic applications.
The distinction between FDA-approved indications and off-label or research-only peptide hgh compounds remains critical for patient safety. Future developments in long-acting formulations and oral secretagogues may expand therapeutic options, but only rigorous clinical testing and regulatory approval can determine their appropriate place in medical practice.
Individuals considering peptide hgh should pursue comprehensive medical evaluation rather than self-administration of unregulated products. Ongoing research through 2026 continues to refine our understanding of optimal dosing, patient selection, and long-term outcomes for this important class of peptides.
Word count: 2487
Peptide HGH encompasses both well-established recombinant therapies with proven efficacy in growth hormone deficiency states and a range of investigational secretagogues that show mechanistic promise but limited long-term safety data for non-approved uses. Current evidence from 2020–2026 strongly supports appropriate medical use in confirmed deficiency while highlighting significant risks and regulatory restrictions for performance, anti-aging, or aesthetic applications.
The distinction between FDA-approved indications and off-label or research-only peptide hgh compounds remains critical for patient safety. Future developments in long-acting formulations and oral secretagogues may expand therapeutic options, but only rigorous clinical testing and regulatory approval can determine their appropriate place in medical practice.
Individuals considering peptide hgh should pursue comprehensive medical evaluation rather than self-administration of unregulated products. Ongoing research through 2026 continues to refine our understanding of optimal dosing, patient selection, and long-term outcomes for this important class of peptides.
Word count: 2487