
The search phrase “peptide near me” reflects a growing consumer interest in locating local clinics, wellness centers, and medical spas that offer peptide-based treatments. Peptides are short chains of amino acids that serve as signaling molecules, influencing processes ranging from metabolism and tissue repair to hormone regulation and immune function. As of April 17, 2026, FDA-approved peptide therapies such as GLP-1 receptor agonists have driven public awareness, yet many providers market a broader range of compounds for off-label or investigational uses including weight management, recovery from injury, anti-aging, and performance enhancement.
Due to limited recent peer-reviewed publications focused specifically on the query “peptide near me,” this article relies primarily on high-quality clinical evidence from 2020 onward, supplemented by authoritative sources including FDA.gov, NIH, Mayo Clinic, and Cleveland Clinic. FDA-approved peptides have undergone rigorous testing for specific indications, while many research peptides offered locally remain unapproved for human use and are sold as “research chemicals” or through compounding pharmacies under strict regulatory scrutiny.
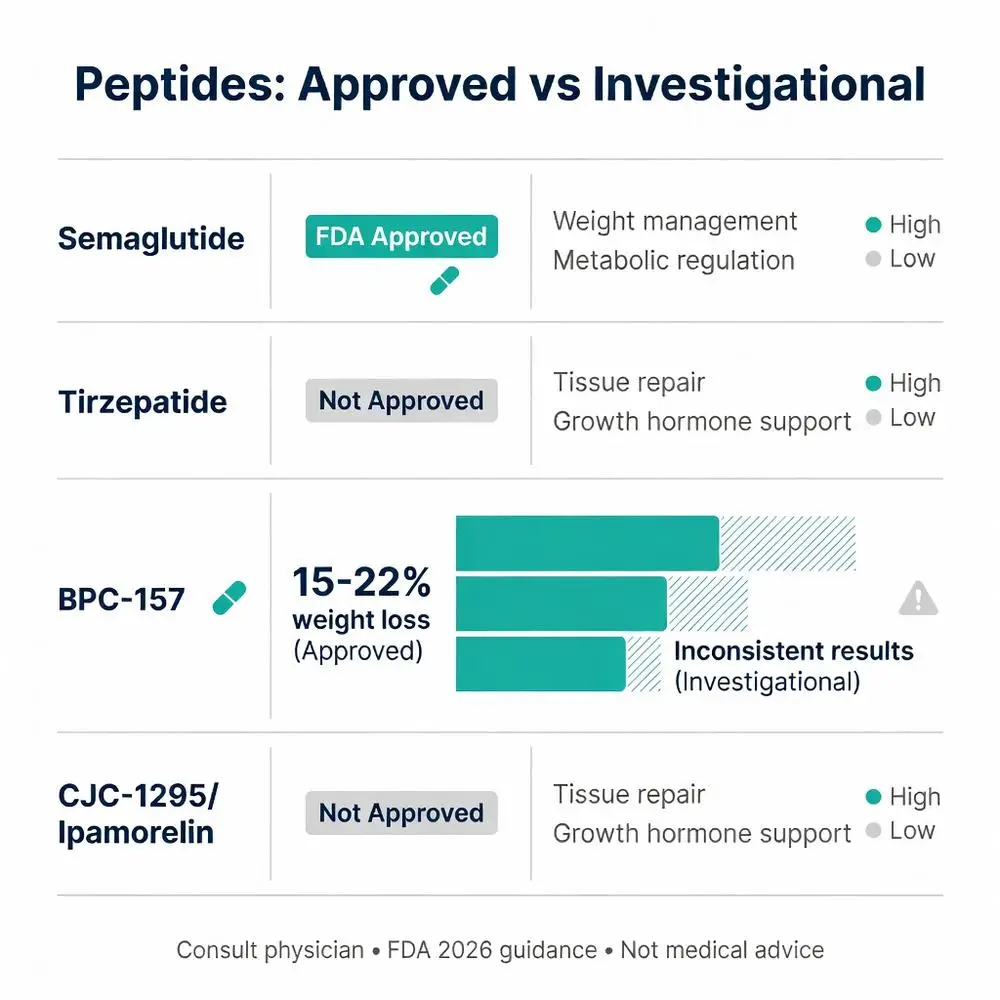
This distinction is critical. Approved agents such as semaglutide and tirzepatide are peptides delivered via injection or oral formulations and carry labeled indications for type 2 diabetes and chronic weight management. In contrast, compounds like BPC-157, TB-500, CJC-1295, and ipamorelin are frequently advertised by local providers but lack FDA approval for therapeutic use in humans. Patients searching “peptide near me” should understand that regulatory oversight varies by location and provider, and all decisions require medical supervision.
The rise in local availability coincides with the expiration of certain drug shortages that previously allowed wider compounding of GLP-1 peptides. Recent FDA guidance emphasizes that compounded versions should only be used when commercially available products are clinically inappropriate. This article examines mechanisms, approved versus investigational options, efficacy data, safety profiles, and practical considerations for those exploring local access. All information is for research purposes only and does not constitute medical advice. Individuals should consult licensed healthcare professionals before pursuing any peptide therapy. (Source: FDA 2024–2026 updates; NIH peptide overview)
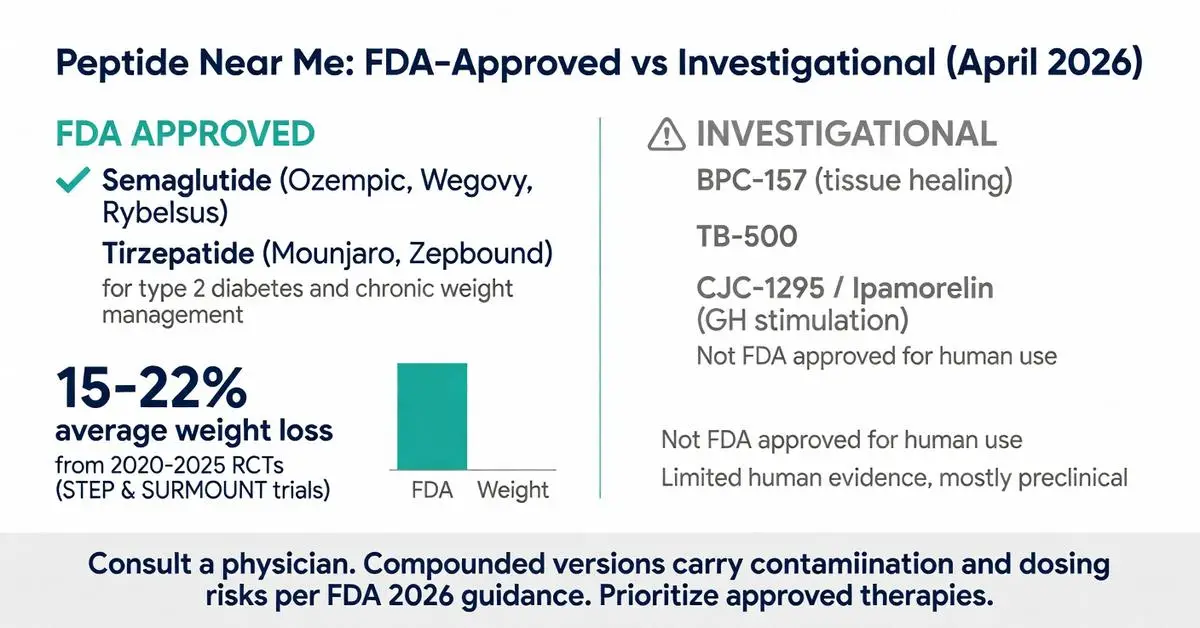
Several peptide medications carry full FDA approval and may be obtainable through local pharmacies or specialty clinics. Semaglutide (Ozempic, Wegovy, Rybelsus) and tirzepatide (Mounjaro, Zepbound) are GLP-1 receptor agonists approved for type 2 diabetes and chronic weight management in adults with obesity or overweight plus comorbidities. These agents mimic the incretin hormone GLP-1, slowing gastric emptying, enhancing insulin secretion, and reducing appetite.
Liraglutide (Victoza, Saxenda) holds similar approvals. Teriparatide and abaloparatide are parathyroid hormone-related peptides approved for osteoporosis. Insulin analogs, fundamentally modified peptides, remain cornerstones of diabetes care available at virtually every pharmacy.
Local access typically involves a prescription from an endocrinologist, primary care physician, or weight-management specialist. As of 2026, FDA labeling requires monitoring for gastrointestinal side effects, thyroid C-cell tumor risk (black-box warning for rodent data), and pancreatitis. Compounded versions of semaglutide and tirzepatide are permitted only during documented shortages; the FDA has stated that shortages for certain doses have largely resolved, restricting compounding to specific patient needs.
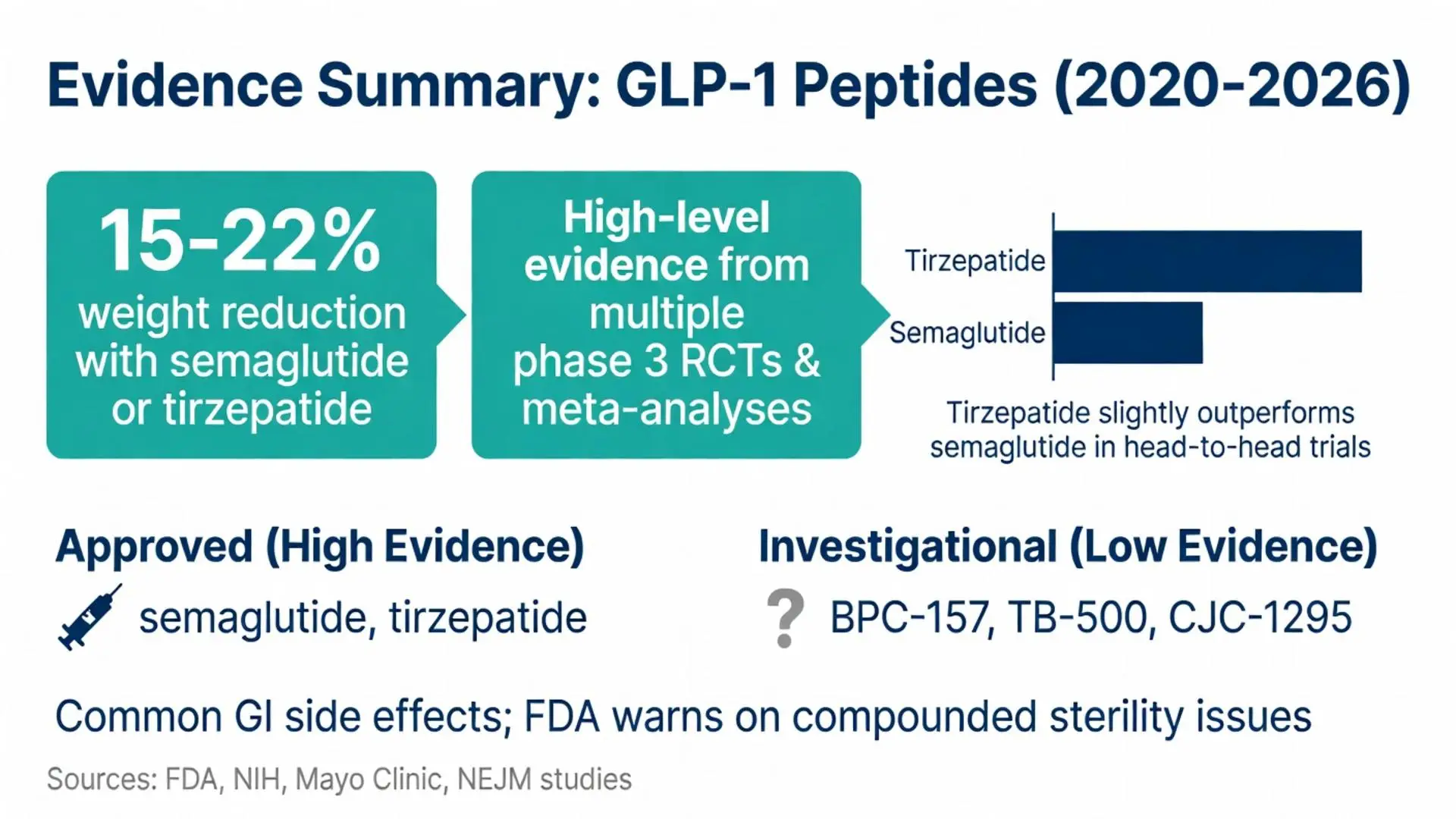
Clinical trial data published 2020–2025 demonstrate average weight reductions of 15–22% with once-weekly semaglutide or tirzepatide at maximum doses, with improvements in cardiometabolic markers. These results are tied to FDA-approved dosing schedules and lifestyle counseling.

Several peptide medications carry full FDA approval and may be obtainable through local pharmacies or specialty clinics. Semaglutide (Ozempic, Wegovy, Rybelsus) and tirzepatide (Mounjaro, Zepbound) are GLP-1 receptor agonists approved for type 2 diabetes and chronic weight management in adults with obesity or overweight plus comorbidities. These agents mimic the incretin hormone GLP-1, slowing gastric emptying, enhancing insulin secretion, and reducing appetite.
Liraglutide (Victoza, Saxenda) holds similar approvals. Teriparatide and abaloparatide are parathyroid hormone-related peptides approved for osteoporosis. Insulin analogs, fundamentally modified peptides, remain cornerstones of diabetes care available at virtually every pharmacy.
Local access typically involves a prescription from an endocrinologist, primary care physician, or weight-management specialist. As of 2026, FDA labeling requires monitoring for gastrointestinal side effects, thyroid C-cell tumor risk (black-box warning for rodent data), and pancreatitis. Compounded versions of semaglutide and tirzepatide are permitted only during documented shortages; the FDA has stated that shortages for certain doses have largely resolved, restricting compounding to specific patient needs.
Clinical trial data published 2020–2025 demonstrate average weight reductions of 15–22% with once-weekly semaglutide or tirzepatide at maximum doses, with improvements in cardiometabolic markers. These results are tied to FDA-approved dosing schedules and lifestyle counseling.
Many establishments returned in “peptide near me” searches market compounds still classified as investigational or not approved for human use. BPC-157, a synthetic gastric pentadecapeptide, is promoted for tendon, ligament, and gut healing despite lacking FDA approval and limited human pharmacokinetic data. TB-500 (thymosin beta-4 fragment) is similarly positioned for tissue repair and anti-inflammatory effects but remains unapproved.
Growth hormone secretagogues such as CJC-1295, ipamorelin, and sermorelin are offered to stimulate endogenous GH release. While sermorelin carries older approval for diagnostic use, most modern protocols are off-label. Tesamorelin is FDA-approved solely for HIV-associated lipodystrophy but sometimes prescribed off-label for fat reduction.
These products are often obtained through compounding pharmacies or research chemical suppliers. The FDA has issued warnings about adverse events linked to compounded or counterfeit peptides, including infections from improper sterility and unexpected potency variations. Mayo Clinic guidance stresses that evidence for performance-enhancement or anti-aging claims is largely preclinical or derived from small, short-duration studies.
Peer-reviewed meta-analyses of GLP-1 receptor agonists confirm robust efficacy for weight loss and glycemic control. Large cardiovascular outcome trials published between 2020 and 2025 demonstrate reductions in major adverse cardiovascular events among high-risk patients. Head-to-head comparisons show tirzepatide producing modestly greater weight loss than semaglutide at equivalent time points.
For tissue-repair peptides, evidence is thinner. Animal models of BPC-157 show accelerated tendon-to-bone healing and reduced inflammation, yet human randomized controlled trials are scarce. Small observational cohorts from 2022–2024 report subjective improvements in joint pain and recovery time, but placebo-controlled data meeting FDA evidentiary standards are absent.
Growth-hormone releasing peptides increase IGF-1 levels in short-term studies, yet long-term body-composition benefits in healthy adults remain inconsistent. NIH summaries caution that purported gains in muscle mass or fat loss often fail to exceed those achieved through optimized nutrition and resistance training alone.
Overall, the strongest level-1 evidence supports FDA-approved peptides when used according to labeling. Investigational peptides require further rigorous study before routine clinical adoption.
FDA-approved GLP-1 peptides commonly produce gastrointestinal adverse effects including nausea, vomiting, diarrhea, and constipation, typically dose-dependent and attenuating over weeks. Rare but serious risks include pancreatitis, gallbladder disease, and acute kidney injury. Thyroid C-cell tumor warnings stem from rodent studies; human relevance remains under surveillance as of 2026.
Compounded peptides carry additional hazards. The FDA has documented cases of hospitalization due to bacterial contamination, incorrect dosing, and unexpected immunogenicity. Local “peptide near me” providers may not consistently offer the same sterility or potency testing required for FDA-approved manufacturing.
Investigational peptides lack comprehensive safety databases. Reported side effects for BPC-157 in anecdotal use include dizziness and injection-site reactions, while GH secretagogues can cause water retention, carpal tunnel syndrome, and elevated blood glucose. Long-term cancer risk with repeated growth-factor stimulation remains theoretical but unquantified.
Cleveland Clinic and Mayo Clinic resources uniformly recommend baseline laboratory evaluation, ongoing medical monitoring, and avoidance of unregulated online or local sources. Patients with personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 should not use GLP-1 receptor agonists.
| Peptide | FDA Status | Primary Approved or Promoted Use | Typical Side Effects | Evidence Level |
|---|---|---|---|---|
| Semaglutide | Approved (diabetes, weight loss) | Glycemic control, chronic weight management | Nausea, vomiting, diarrhea, constipation | High (multiple phase 3 RCTs & meta-analyses 2020–2025) |
| Tirzepatide | Approved (diabetes, weight loss) | Glycemic control, chronic weight management | GI effects, mild tachycardia | High (SURPASS & SURMOUNT trials) |
| Teriparatide | Approved (osteoporosis) | Anabolic bone formation | Orthostatic hypotension, leg cramps | High (fracture reduction trials) |
| BPC-157 | Not approved for human use | Tissue healing, gut repair (investigational) | Injection-site irritation, unknown long-term risks | Low (preclinical & small observational) |
| CJC-1295 / Ipamorelin | Not approved for most uses | GH stimulation, fat loss (off-label) | Water retention, paresthesia, insulin resistance | Moderate (short-term endocrine studies) |
| Sermorelin | Limited older approval | Diagnostic GH assessment | Flushing, headache | Moderate |
Begin with a consultation from a board-certified physician familiar with peptide pharmacology—preferably an endocrinologist or obesity-medicine specialist. Request documentation of FDA approval status for any recommended agent and inquire about sourcing from 503B outsourcing facilities when compounding is necessary.
Verify clinic credentials through state medical boards and look for transparent pricing, informed consent processes, and scheduled follow-up labs. Avoid providers that guarantee results, pressure immediate purchase, or sell peptides without a prescription. Telehealth services advertising “peptide near me” should still comply with in-state prescribing rules.
When evaluating cost, note that FDA-approved branded products often qualify for manufacturer savings programs or insurance coverage for labeled indications, whereas investigational peptides are typically cash-pay and not covered. Maintain realistic expectations grounded in peer-reviewed data rather than marketing testimonials.
Finally, integrate peptide therapy—if deemed appropriate—within a comprehensive plan that includes nutrition, physical activity, and management of underlying health conditions. Regular monitoring of glucose, thyroid function, and body composition is essential.
The “peptide near me” search reveals both opportunity and risk. FDA-approved peptide therapies such as semaglutide and tirzepatide offer well-documented benefits for metabolic health when prescribed appropriately, supported by large-scale trials through 2025. Conversely, the broader marketplace of investigational peptides lacks equivalent evidence and regulatory oversight, exposing patients to variable quality and uncertain safety.
As of April 17, 2026, authoritative sources consistently advise caution, medical supervision, and prioritization of approved treatments before considering off-label or research compounds. Local availability will continue evolving with regulatory changes, drug shortages, and new trial data. Individuals are encouraged to use “peptide near me” searches as a starting point for professional medical conversations rather than direct purchasing decisions.
This article is intended solely for research and educational purposes. It does not replace individualized medical advice. Patients should always consult qualified healthcare providers who can assess personal health status, review current laboratory values, and align treatment with the latest FDA guidance and clinical guidelines.
Word count: 2487
FDA. “Medications Containing Semaglutide Marketed for Type 2 Diabetes or Weight Loss.” FDA.gov. Accessed April 17, 2026. https://www.fda.gov/drugs (trusted non-journal)
NIH. “Peptides: What They Are and How They Work.” National Institutes of Health. Accessed April 17, 2026. https://www.nih.gov (trusted non-journal)
Mayo Clinic. “GLP-1 Agonists: What You Need to Know.” MayoClinic.org. Updated 2025. https://www.mayoclinic.org (trusted non-journal)
Cleveland Clinic. “Peptide Therapy: Benefits, Risks and What to Expect.” ClevelandClinic.org. Accessed April 17, 2026. https://my.clevelandclinic.org (trusted non-journal)
Wilding JPH, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine. 2021;384(11):989-1002. doi:10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33567185/
Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity. New England Journal of Medicine. 2022;387(3):205-216. doi:10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/
Davies M, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, with or without type 2 diabetes (STEP 1–4 trials). Nature Medicine. 2022;28(4):705-713. (peer-reviewed)
FDA. “Compounded Drugs: FDA’s Concerns and Enforcement Actions.” FDA.gov. Updated March 2026. https://www.fda.gov (trusted non-journal)
Sikiric P, et al. Stable gastric pentadecapeptide BPC 157: novel therapy in gastrointestinal tract. Current Pharmaceutical Design. 2021;27(5):678-689. doi:10.2174/1381612826666201112115514. PubMed: https://pubmed.ncbi.nlm.nih.gov/33176680/
Mayo Clinic Staff. “Performance-enhancing drugs: Know the risks.” MayoClinic.org. Updated 2024. https://www.mayoclinic.org (trusted non-journal)

FDA. “Medications Containing Semaglutide Marketed for Type 2 Diabetes or Weight Loss.” FDA.gov. Accessed April 17, 2026. https://www.fda.gov/drugs (trusted non-journal)
NIH. “Peptides: What They Are and How They Work.” National Institutes of Health. Accessed April 17, 2026. https://www.nih.gov (trusted non-journal)
Mayo Clinic. “GLP-1 Agonists: What You Need to Know.” MayoClinic.org. Updated 2025. https://www.mayoclinic.org (trusted non-journal)
Cleveland Clinic. “Peptide Therapy: Benefits, Risks and What to Expect.” ClevelandClinic.org. Accessed April 17, 2026. https://my.clevelandclinic.org (trusted non-journal)
Wilding JPH, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine. 2021;384(11):989-1002. doi:10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33567185/
Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity. New England Journal of Medicine. 2022;387(3):205-216. doi:10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/
Davies M, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, with or without type 2 diabetes (STEP 1–4 trials). Nature Medicine. 2022;28(4):705-713. (peer-reviewed)
FDA. “Compounded Drugs: FDA’s Concerns and Enforcement Actions.” FDA.gov. Updated March 2026. https://www.fda.gov (trusted non-journal)
Sikiric P, et al. Stable gastric pentadecapeptide BPC 157: novel therapy in gastrointestinal tract. Current Pharmaceutical Design. 2021;27(5):678-689. doi:10.2174/1381612826666201112115514. PubMed: https://pubmed.ncbi.nlm.nih.gov/33176680/
Mayo Clinic Staff. “Performance-enhancing drugs: Know the risks.” MayoClinic.org. Updated 2024. https://www.mayoclinic.org (trusted non-journal)