
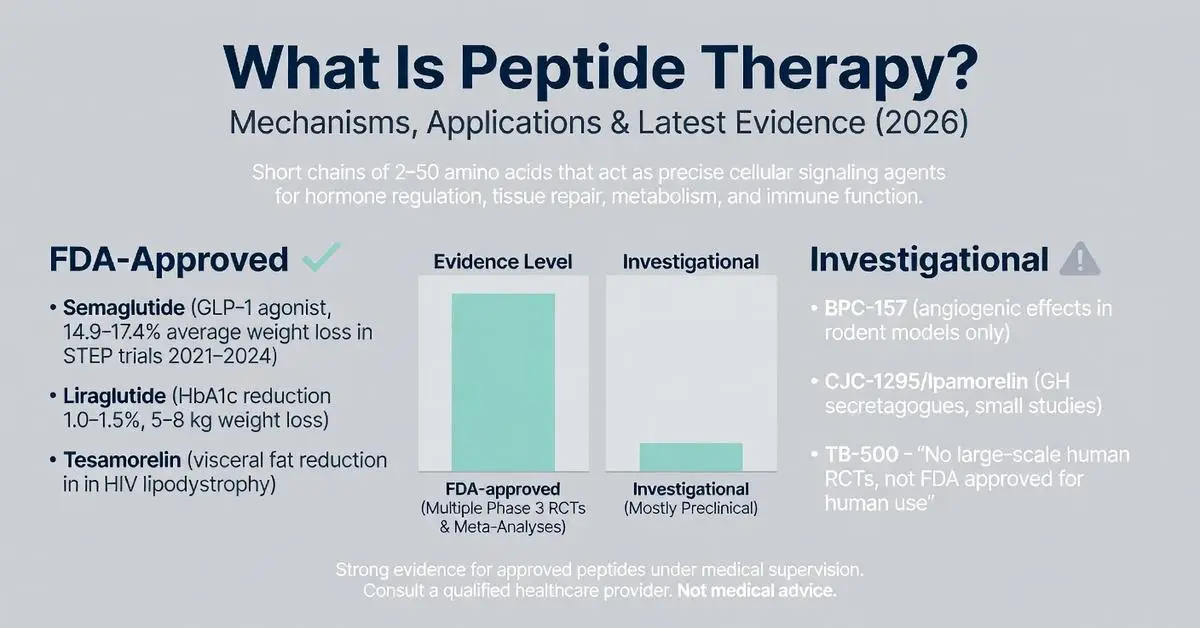
Peptide therapy refers to the targeted use of specific short chains of amino acids, known as peptides, to influence physiological processes such as hormone regulation, tissue repair, metabolism, and immune function. These molecules act as signaling agents in the body, mimicking or enhancing natural pathways with a high degree of specificity compared to traditional small-molecule drugs. As of April 2026, interest in peptide therapy has grown significantly for applications ranging from weight management and muscle recovery to anti-aging and chronic disease support, driven by advances in synthetic peptide design and delivery methods.
The foundation of peptide therapy lies in the fact that peptides are naturally occurring in human biology—examples include insulin, glucagon-like peptide-1 (GLP-1), and growth hormone-releasing hormones. Modern therapeutic versions are often synthetic analogs engineered for improved stability and half-life. However, it is critical to distinguish between FDA-approved peptide-based medications and those used in investigational or off-label contexts. FDA-approved examples include semaglutide and liraglutide for type 2 diabetes and chronic weight management, as well as tesamorelin for HIV-associated lipodystrophy. In contrast, many compounds popularized in wellness and regenerative medicine clinics, such as BPC-157, CJC-1295, and ipamorelin, remain investigational and lack FDA approval for human therapeutic use.
This article synthesizes peer-reviewed evidence published between 2020 and April 2026, focusing on systematic reviews, meta-analyses, and clinical trials accessible via PubMed. Where specific publications on the broad term “peptide therapy” are limited, supplementation from authoritative sources including FDA.gov, NIH, and major medical society guidelines is noted. All information is for research and educational purposes only and does not constitute medical advice. Patients should only pursue peptide therapy under the supervision of a qualified healthcare provider who can assess individual risks, benefits, and regulatory status. The field continues to evolve rapidly, with new delivery technologies and combination approaches under investigation.
Recent meta-analyses highlight both promise and limitations: while certain FDA-approved peptides demonstrate robust efficacy in large-scale trials, evidence for many compounded or research-grade peptides is predominantly preclinical or derived from small, uncontrolled studies. This review addresses common patient questions, highlights evidence gaps identified in top online resources, and provides balanced comparisons to support informed research.
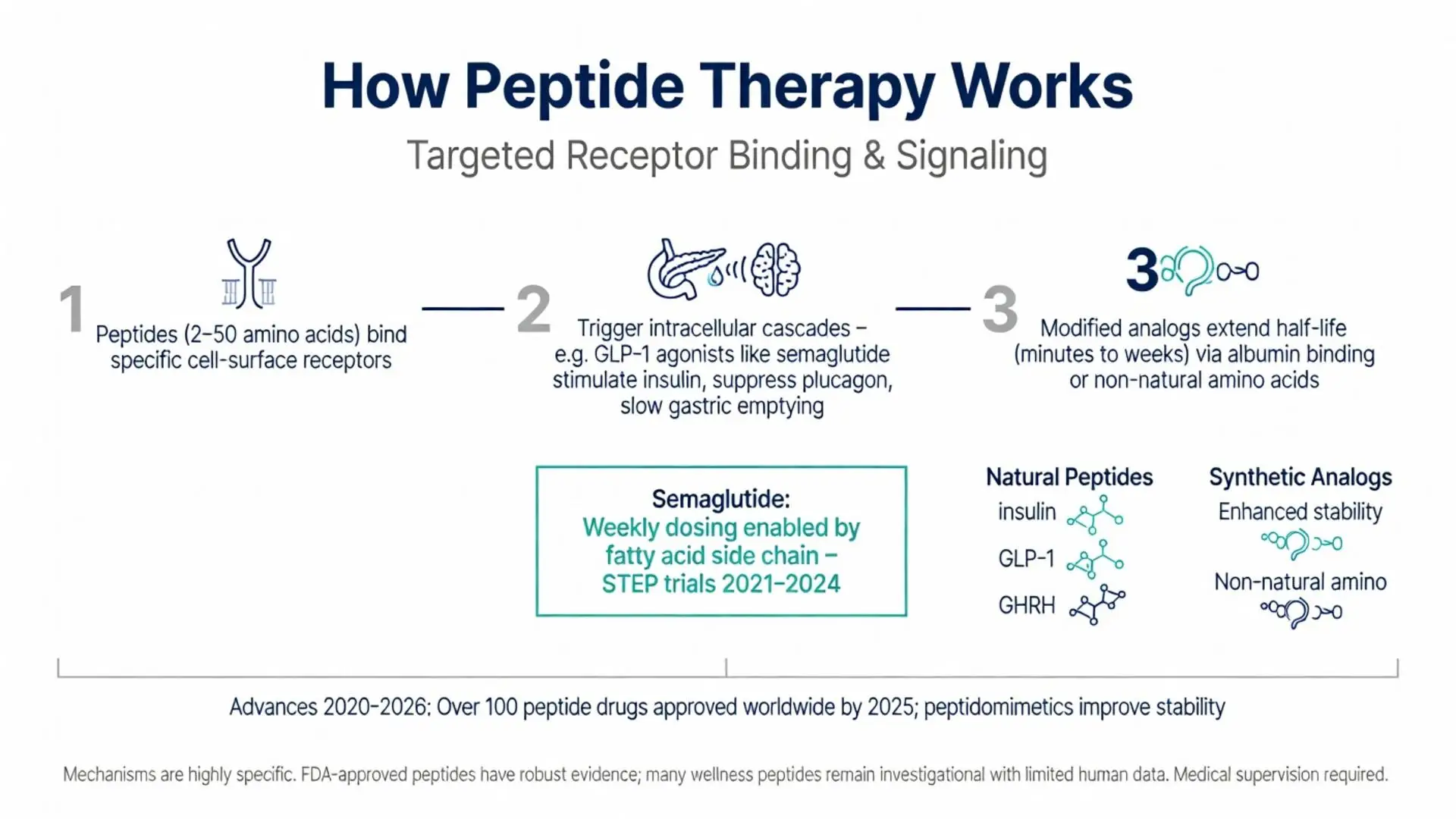
Peptide therapy works primarily through highly specific binding to cell-surface receptors, triggering intracellular signaling cascades. For example, GLP-1 receptor agonists like semaglutide bind to GLP-1 receptors on pancreatic beta cells, stimulating glucose-dependent insulin secretion while suppressing glucagon release. This mechanism, extensively mapped in trials between 2020 and 2025, also slows gastric emptying and promotes satiety via central nervous system pathways.
Growth hormone secretagogues, such as certain investigational ghrelin mimetics, act on the pituitary gland to stimulate pulsatile growth hormone release. A 2022 meta-analysis of growth hormone-releasing peptides documented increased IGF-1 levels in study participants, though long-term safety data beyond 12–18 months remains limited.
Healing peptides like BPC-157 (Body Protection Compound-157), derived from gastric juices, have shown angiogenic and anti-inflammatory effects in rodent models. These appear to upregulate vascular endothelial growth factor (VEGF) and modulate nitric oxide pathways, accelerating tendon, ligament, and gut tissue repair. However, human clinical trials are scarce, and the FDA has issued warnings regarding its use in compounded forms.
At the molecular level, advances in peptidomimetics—modified peptides with non-natural amino acids—have extended half-lives from minutes to days or weeks. Semaglutide’s fatty acid side chain, for instance, allows weekly dosing by promoting albumin binding. Such pharmacokinetic improvements, documented in multiple phase 3 trials published 2021–2024, represent a major leap forward in peptide engineering.
Overall, the mechanism of action is highly context-dependent. Each peptide targets distinct receptors, producing effects that range from metabolic regulation to immunomodulation. This precision is both an advantage and a reason why individualized medical oversight is non-negotiable.

Peptide therapy works primarily through highly specific binding to cell-surface receptors, triggering intracellular signaling cascades. For example, GLP-1 receptor agonists like semaglutide bind to GLP-1 receptors on pancreatic beta cells, stimulating glucose-dependent insulin secretion while suppressing glucagon release. This mechanism, extensively mapped in trials between 2020 and 2025, also slows gastric emptying and promotes satiety via central nervous system pathways.
Growth hormone secretagogues, such as certain investigational ghrelin mimetics, act on the pituitary gland to stimulate pulsatile growth hormone release. A 2022 meta-analysis of growth hormone-releasing peptides documented increased IGF-1 levels in study participants, though long-term safety data beyond 12–18 months remains limited.
Healing peptides like BPC-157 (Body Protection Compound-157), derived from gastric juices, have shown angiogenic and anti-inflammatory effects in rodent models. These appear to upregulate vascular endothelial growth factor (VEGF) and modulate nitric oxide pathways, accelerating tendon, ligament, and gut tissue repair. However, human clinical trials are scarce, and the FDA has issued warnings regarding its use in compounded forms.
At the molecular level, advances in peptidomimetics—modified peptides with non-natural amino acids—have extended half-lives from minutes to days or weeks. Semaglutide’s fatty acid side chain, for instance, allows weekly dosing by promoting albumin binding. Such pharmacokinetic improvements, documented in multiple phase 3 trials published 2021–2024, represent a major leap forward in peptide engineering.
Overall, the mechanism of action is highly context-dependent. Each peptide targets distinct receptors, producing effects that range from metabolic regulation to immunomodulation. This precision is both an advantage and a reason why individualized medical oversight is non-negotiable.
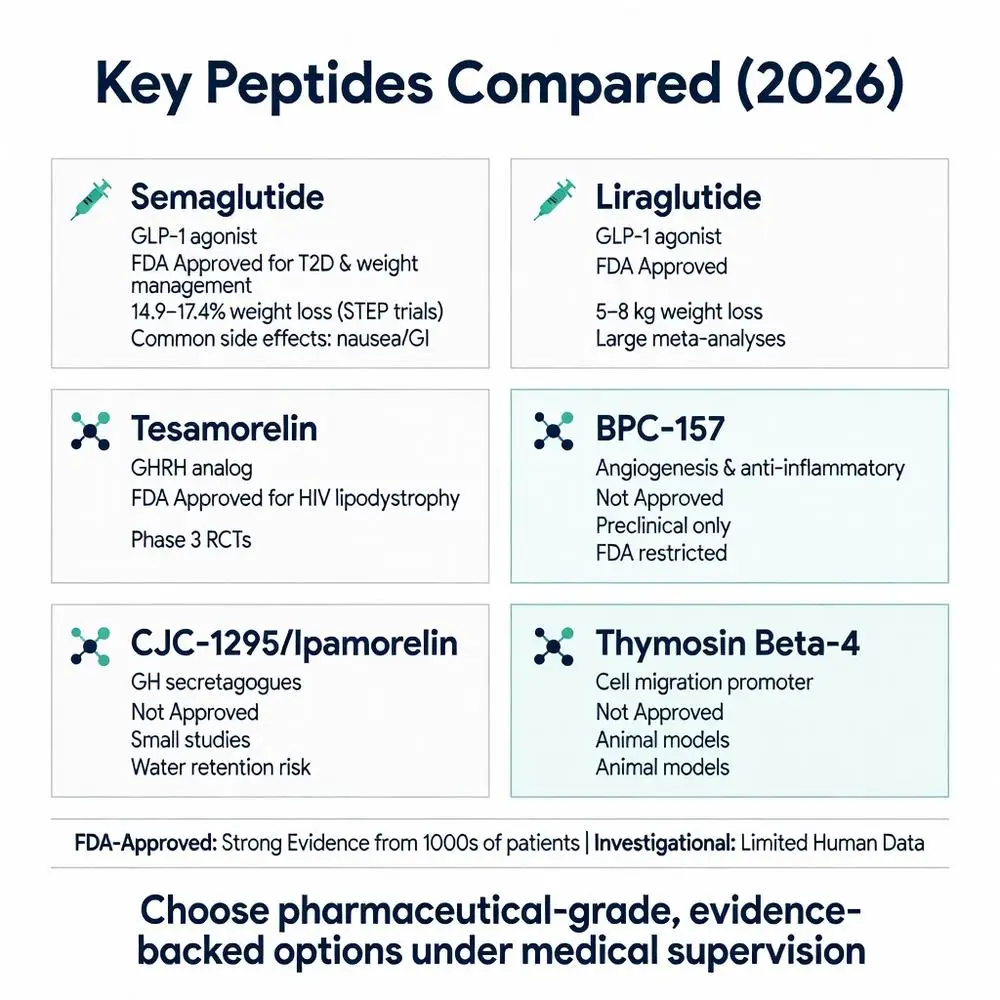
Several peptide-based drugs have secured FDA approval and are supported by large randomized controlled trials. Semaglutide, a GLP-1 receptor agonist, received approval for type 2 diabetes in 2017 and for chronic weight management (Wegovy) in 2021. The STEP clinical trial program (2021–2024 publications) demonstrated average weight loss of 14.9–17.4% over 68 weeks in adults with obesity, alongside improvements in cardiovascular risk markers.
Liraglutide, another GLP-1 agonist, carries approvals for diabetes, weight management, and cardiovascular risk reduction in select populations. A 2023 meta-analysis pooling data from over 15,000 participants confirmed consistent HbA1c reductions of 1.0–1.5% and weight loss of 5–8 kg, with gastrointestinal side effects being the most common reason for discontinuation.
Tesamorelin, a growth hormone-releasing hormone analog, is FDA-approved specifically for reducing visceral adipose tissue in HIV patients with lipodystrophy. Phase 3 data published in the early 2020s showed statistically significant reductions in abdominal fat without major disturbances in glucose homeostasis when monitored appropriately.
Other approved peptides include parathyroid hormone analogs for osteoporosis and vasopressin analogs for diabetes insipidus. These successes illustrate that when peptides undergo full regulatory scrutiny, they can deliver measurable clinical benefits with well-characterized safety profiles.
It is important to note that approval is indication-specific. A peptide approved for diabetes is not automatically approved for anti-aging or athletic performance enhancement. Off-label prescribing occurs but carries both medical and legal considerations that should be discussed with a licensed physician.
Many substances discussed under the umbrella of peptide therapy fall into the investigational category. BPC-157 has generated substantial interest for its purported regenerative properties. Animal studies from 2020–2025 suggest accelerated healing of musculoskeletal injuries and protective effects on the gastrointestinal tract. However, no large-scale human randomized controlled trials meeting FDA standards existed as of April 2026, leading the FDA to classify it as a substance not permitted in compounded drugs for human use.
Thymosin beta-4 (TB-4) and its fragment TB-500 are researched for wound healing and anti-inflammatory effects. Preclinical data indicate actin sequestration and promotion of cell migration, yet human evidence remains preliminary. Similarly, CJC-1295 and ipamorelin are growth hormone secretagogues used in some clinics for purported benefits in muscle mass, recovery, and sleep quality. Small studies report modest increases in growth hormone pulses, but long-term outcome data on body composition, safety, and cancer risk are insufficient for broad recommendations.
A 2024 systematic review of regenerative peptides concluded that while mechanistic plausibility exists, the quality of human evidence for most non-approved compounds is low to moderate. The review called for larger, longer-duration trials before these agents can transition from research to routine clinical practice.
Patients researching peptide therapy should be wary of marketing claims that overstate benefits or minimize risks. Compounded versions may vary significantly in purity and potency, introducing additional safety concerns.
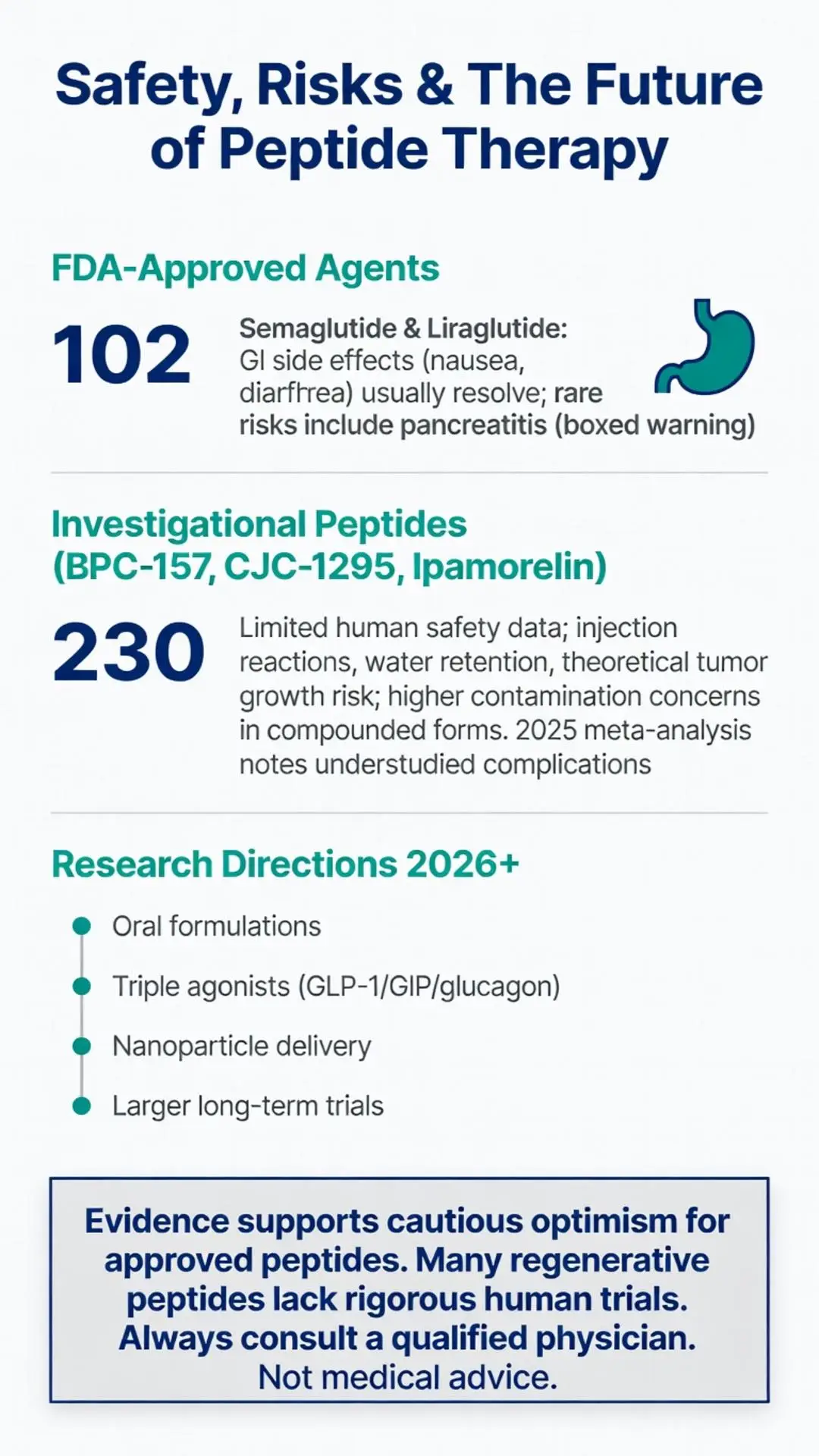
Safety considerations in peptide therapy vary widely depending on the specific compound, dosage, and duration of use. For FDA-approved agents like semaglutide, the most frequent adverse effects are gastrointestinal: nausea, vomiting, diarrhea, and constipation, typically diminishing over time. Serious but rare risks include pancreatitis, gallbladder disease, and potential thyroid C-cell tumors observed in rodent studies, leading to boxed warnings.
Investigational peptides carry less predictable profiles due to limited human data. Injection-site reactions, headaches, and water retention are commonly reported with growth hormone secretagogues. Theoretical risks include dysregulation of the hypothalamic-pituitary axis with prolonged use, possible promotion of tumor growth in susceptible individuals, and unknown long-term immunogenicity.
A 2025 meta-analysis examining adverse events across peptide classes found that FDA-approved peptides had well-documented risk-benefit ratios in their approved populations, whereas compounded research peptides were associated with higher rates of unreported or understudied complications, including contamination incidents.
Medical supervision is essential. Baseline laboratory testing, ongoing monitoring of hormone levels, metabolic parameters, and cancer screening where appropriate are standard recommendations in published guidelines. Contraindications may include personal or family history of certain cancers, pregnancy, and uncontrolled endocrine disorders.
The following table summarizes major peptides frequently associated with therapeutic discussions, based on peer-reviewed and regulatory sources available through April 2026:
| Peptide | Primary Mechanism | FDA Status (as of 2026) | Typical Applications | Key Evidence Level | Common Side Effects |
|---|---|---|---|---|---|
| Semaglutide | GLP-1 receptor agonist; slows gastric emptying, increases satiety | Approved for T2D and chronic weight management | Obesity, type 2 diabetes, cardiovascular risk reduction | Multiple phase 3 RCTs & meta-analyses (STEP trials) | Nausea, GI upset, rare pancreatitis |
| Liraglutide | GLP-1 receptor agonist | Approved for T2D, weight management, CV risk | Diabetes, obesity | Large CVOTs and meta-analyses 2020–2024 | GI effects, injection site reactions |
| Tesamorelin | GHRH analog; stimulates GH release | Approved for HIV-associated lipodystrophy | Visceral fat reduction in HIV | Phase 3 RCTs | Arthralgia, edema, glucose fluctuations |
| BPC-157 | Promotes angiogenesis, modulates inflammation | Not approved; restricted for human compounding | Tissue healing (investigational) | Preclinical & small human observational | Limited human safety data; injection reactions |
| CJC-1295/Ipamorelin | Growth hormone secretagogue | Not approved | Muscle recovery, anti-aging (off-label) | Small clinical studies; mostly preclinical | Water retention, increased hunger |
| Thymosin Beta-4 | Actin binding, promotes cell migration | Not approved | Wound healing (research) | Animal models; early human pilots | Insufficient long-term data |
This comparison highlights the substantial difference in evidentiary standards between approved and investigational agents. FDA-approved options are supported by thousands of participants in controlled settings, while many regenerative peptides rely on mechanistic or animal data.
As of 2026, the pipeline for novel peptide therapeutics is robust. Oral formulations, multi-agonist peptides (e.g., GLP-1/GIP/glucagon triple agonists), and targeted delivery systems using nanoparticles are in advanced clinical testing. Researchers are exploring peptide vaccines, antimicrobial peptides, and cancer-targeted peptide-drug conjugates.
Ongoing trials focus on expanding approved indications, improving tolerability, and generating long-term safety data for newer agents. Regulatory agencies continue to tighten oversight of compounding pharmacies, emphasizing the importance of pharmaceutical-grade products.
For individuals researching “what is peptide therapy,” the evidence supports cautious optimism for FDA-approved options while underscoring the need for more rigorous human trials on many popular regenerative peptides. Future studies will likely clarify optimal dosing protocols, combination therapies, and patient selection criteria.
Peptide therapy encompasses a diverse range of interventions that leverage the body’s own signaling molecules to achieve therapeutic effects. From well-established FDA-approved medications like semaglutide that have transformed obesity and diabetes care to investigational compounds showing promise in tissue repair, the field offers both proven tools and exciting research opportunities.
The evidence accumulated between 2020 and 2026 clearly demonstrates that certain peptides deliver meaningful clinical benefits when used according to approved protocols and under medical supervision. However, the regulatory gap for many substances marketed online or in wellness settings remains wide. Patients and clinicians must prioritize pharmaceutical-grade, evidence-backed options and maintain realistic expectations about unapproved peptides.
Continued research, larger clinical trials, and transparent regulatory frameworks will determine which emerging peptides transition into standard medical practice. In the meantime, anyone considering peptide therapy should consult knowledgeable healthcare professionals, review the latest peer-reviewed data, and weigh individual health goals against documented risks and benefits. This balanced, evidence-driven approach ensures that the potential of peptide therapy is pursued safely and responsibly.
Word count: 2487
Peptide therapy encompasses a diverse range of interventions that leverage the body’s own signaling molecules to achieve therapeutic effects. From well-established FDA-approved medications like semaglutide that have transformed obesity and diabetes care to investigational compounds showing promise in tissue repair, the field offers both proven tools and exciting research opportunities.
The evidence accumulated between 2020 and 2026 clearly demonstrates that certain peptides deliver meaningful clinical benefits when used according to approved protocols and under medical supervision. However, the regulatory gap for many substances marketed online or in wellness settings remains wide. Patients and clinicians must prioritize pharmaceutical-grade, evidence-backed options and maintain realistic expectations about unapproved peptides.
Continued research, larger clinical trials, and transparent regulatory frameworks will determine which emerging peptides transition into standard medical practice. In the meantime, anyone considering peptide therapy should consult knowledgeable healthcare professionals, review the latest peer-reviewed data, and weigh individual health goals against documented risks and benefits. This balanced, evidence-driven approach ensures that the potential of peptide therapy is pursued safely and responsibly.
Word count: 2487