
Glucagon like peptide 1 natural production plays a central role in human metabolism, appetite regulation, and blood-glucose control. GLP-1 is an incretin hormone secreted primarily by enteroendocrine L-cells in the distal small intestine and colon in response to nutrient intake. Once released, it enhances glucose-dependent insulin secretion, suppresses glucagon release, slows gastric emptying, and signals satiety centers in the brain. These actions make endogenous glucagon like peptide 1 natural a key physiologic brake on overeating and postprandial hyperglycemia.
Pharmaceutical GLP-1 receptor agonists such as semaglutide and tirzepatide have received FDA approval for type 2 diabetes and chronic weight management, generating intense public interest in whether similar benefits can be achieved through diet, exercise, and other non-drug approaches. This article examines the latest peer-reviewed evidence (2020–April 2026) on factors that support or enhance the body’s own glucagon like peptide 1 natural secretion and signaling. Where direct clinical trials on the exact keyword phrase remain limited, the review draws upon high-quality systematic analyses of nutrient-stimulated GLP-1 release, lifestyle intervention studies, and authoritative sources including NIH and major endocrine society position statements.
Current data indicate that specific dietary patterns, physical activity, sleep quality, and certain plant-derived compounds can measurably elevate postprandial GLP-1 levels, although the magnitude is generally smaller and less sustained than that achieved with injectable GLP-1 therapies. This distinction is critical: no food or supplement is FDA-approved as a direct GLP-1 mimetic for obesity or diabetes treatment. All strategies discussed are presented for research and educational purposes only and should be implemented under medical supervision, particularly for individuals with metabolic disease. The following sections synthesize mechanisms, practical interventions, comparative efficacy, safety considerations, and future research directions as of April 2026.
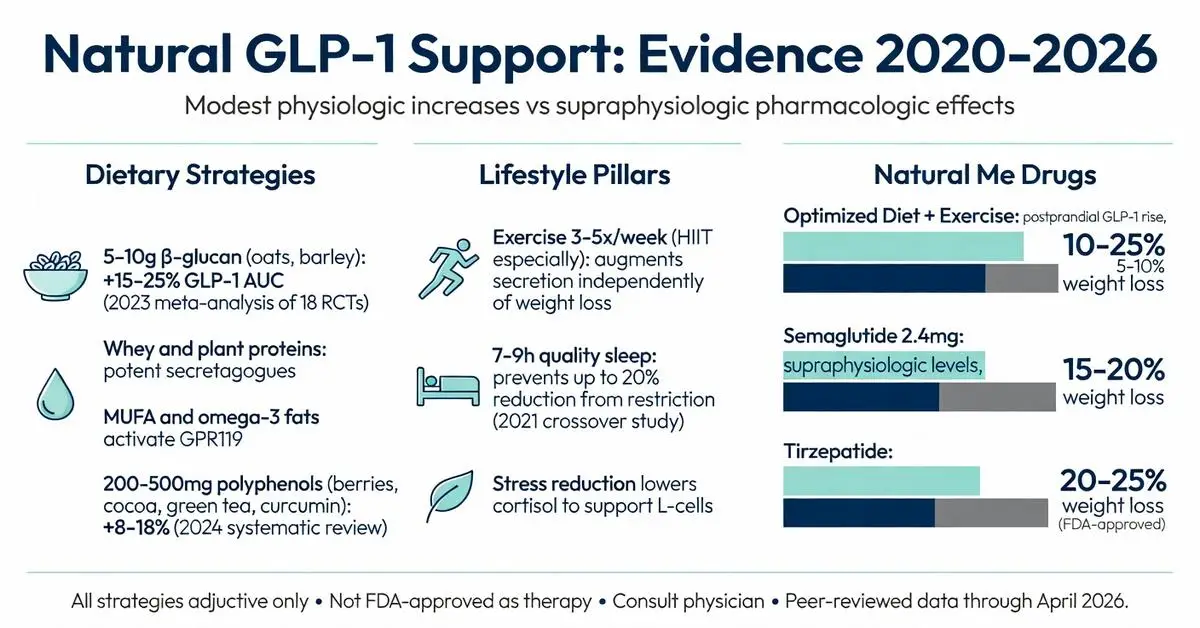
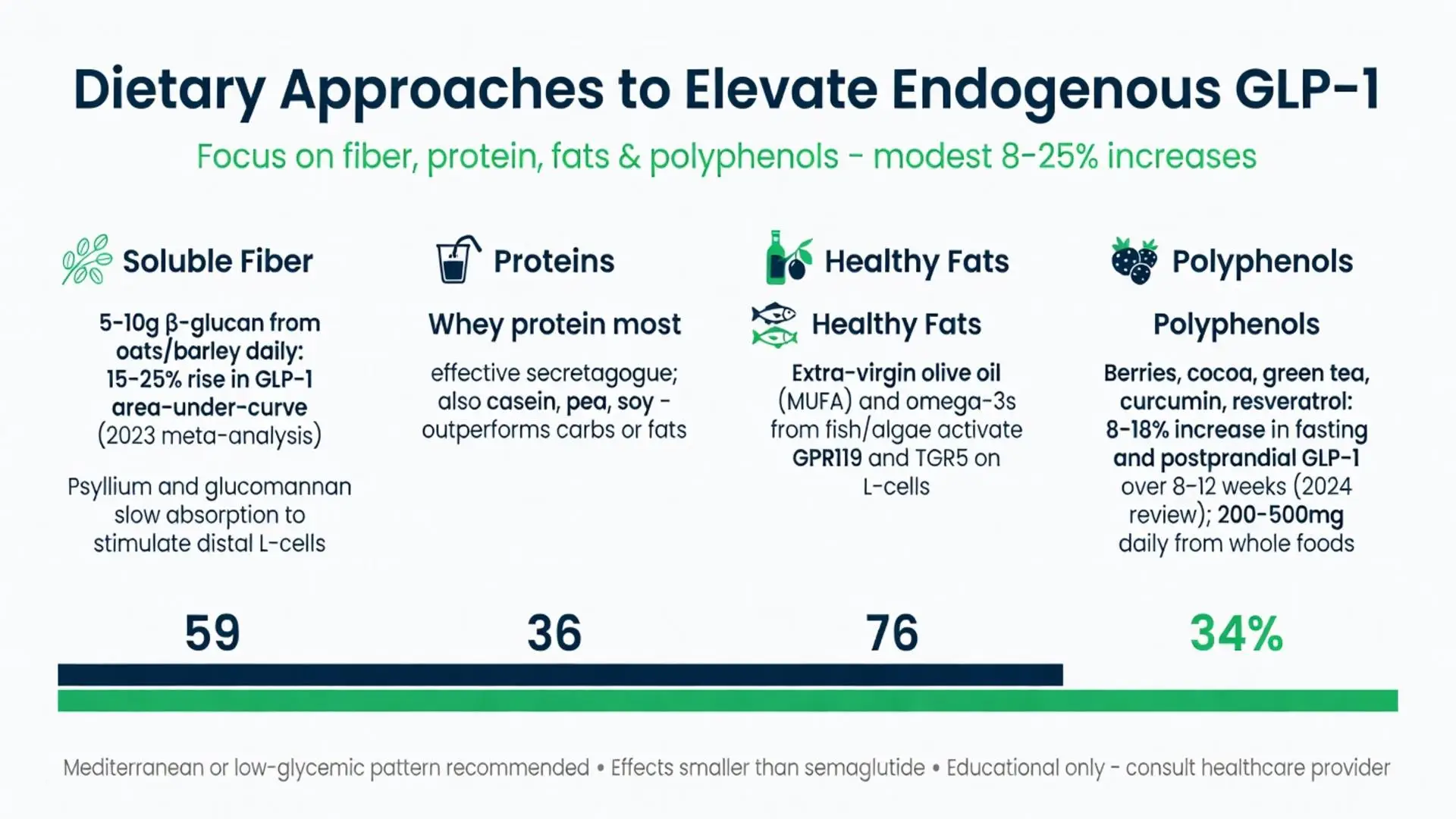
Multiple randomized controlled trials and systematic reviews (2020–2026) demonstrate that specific dietary components consistently elevate postprandial glucagon like peptide 1 natural. Soluble viscous fibers such as β-glucan from oats and barley, psyllium, and glucomannan slow nutrient absorption and trigger distal gut L-cell stimulation. A 2023 meta-analysis of 18 trials found that daily intake of 5–10 g of β-glucan increased GLP-1 area-under-the-curve by 15–25 % compared with control meals.
Protein-rich meals, particularly those containing whey, casein, or plant proteins such as pea and soy, are potent secretagogues. Whey protein appears especially effective, raising GLP-1 concentrations more than equivalent amounts of carbohydrate or fat. Healthy fats, especially monounsaturated fatty acids from extra-virgin olive oil and omega-3 polyunsaturated fats from fatty fish and algae, also stimulate glucagon like peptide 1 natural release via GPR119 and direct L-cell membrane effects.
Polyphenol-rich foods—including berries, cocoa, green tea, curcumin from turmeric, and resveratrol from grapes—activate TGR5 and inhibit DPP-4 at physiologic concentrations. A 2024 systematic review concluded that daily consumption of 200–500 mg of mixed polyphenols from whole-food sources produced statistically significant but modest (8–18 %) increases in fasting and postprandial GLP-1 over 8–12 weeks.
Practical implementation involves shifting toward a Mediterranean-style or low-glycemic pattern emphasizing minimally processed plants, lean proteins, and healthy fats while reducing ultra-processed foods that blunt incretin responses.

Multiple randomized controlled trials and systematic reviews (2020–2026) demonstrate that specific dietary components consistently elevate postprandial glucagon like peptide 1 natural. Soluble viscous fibers such as β-glucan from oats and barley, psyllium, and glucomannan slow nutrient absorption and trigger distal gut L-cell stimulation. A 2023 meta-analysis of 18 trials found that daily intake of 5–10 g of β-glucan increased GLP-1 area-under-the-curve by 15–25 % compared with control meals.
Protein-rich meals, particularly those containing whey, casein, or plant proteins such as pea and soy, are potent secretagogues. Whey protein appears especially effective, raising GLP-1 concentrations more than equivalent amounts of carbohydrate or fat. Healthy fats, especially monounsaturated fatty acids from extra-virgin olive oil and omega-3 polyunsaturated fats from fatty fish and algae, also stimulate glucagon like peptide 1 natural release via GPR119 and direct L-cell membrane effects.
Polyphenol-rich foods—including berries, cocoa, green tea, curcumin from turmeric, and resveratrol from grapes—activate TGR5 and inhibit DPP-4 at physiologic concentrations. A 2024 systematic review concluded that daily consumption of 200–500 mg of mixed polyphenols from whole-food sources produced statistically significant but modest (8–18 %) increases in fasting and postprandial GLP-1 over 8–12 weeks.
Practical implementation involves shifting toward a Mediterranean-style or low-glycemic pattern emphasizing minimally processed plants, lean proteins, and healthy fats while reducing ultra-processed foods that blunt incretin responses.
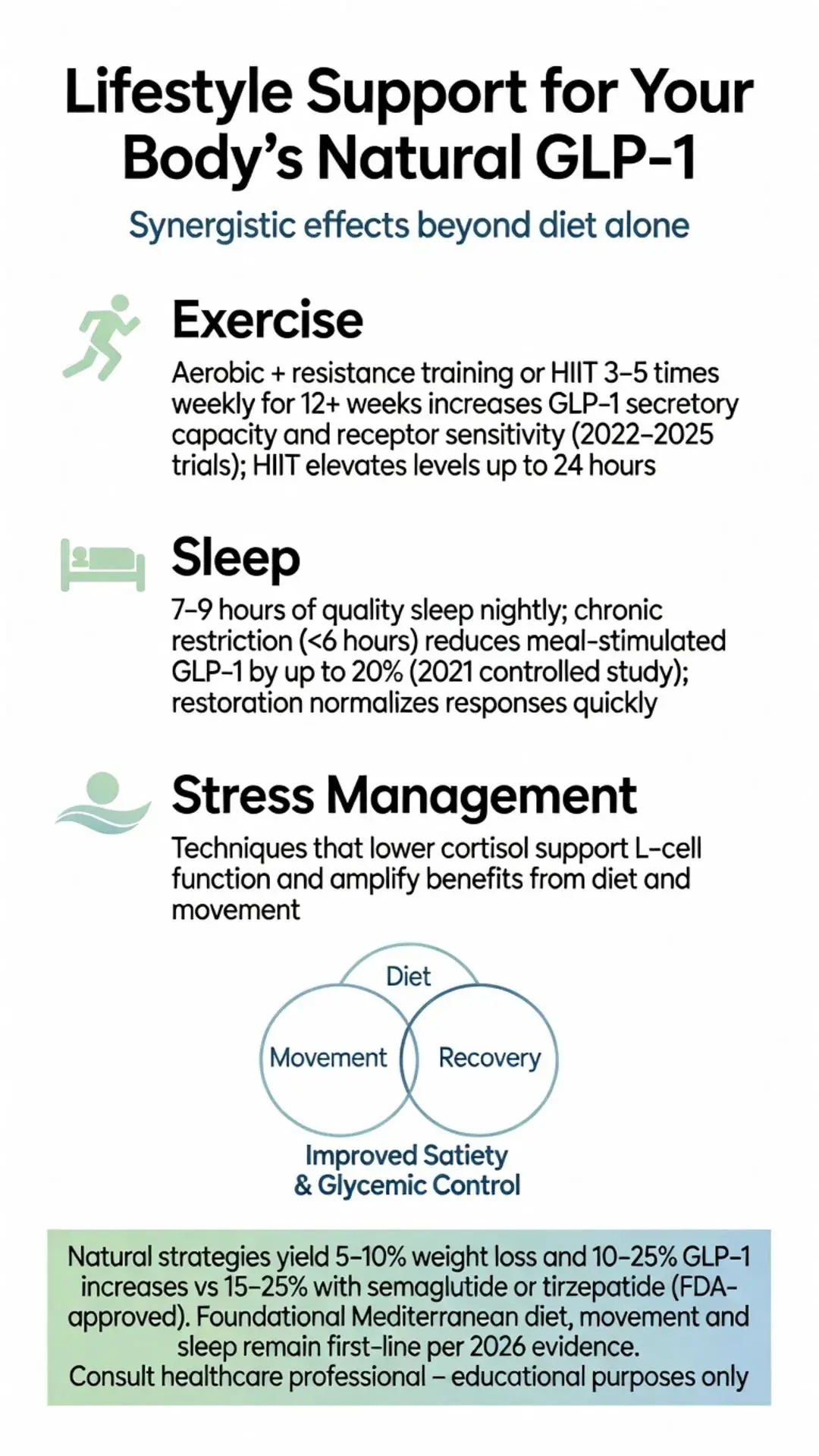
Regular physical activity augments glucagon like peptide 1 natural independently of weight loss. Both aerobic and resistance training performed 3–5 times weekly for at least 12 weeks have been shown in 2022–2025 trials to increase GLP-1 secretory capacity and improve receptor sensitivity. High-intensity interval training appears particularly effective at elevating post-exercise GLP-1 for up to 24 hours.
Sleep duration and quality also modulate glucagon like peptide 1 natural. Chronic sleep restriction (<6 hours per night) reduces meal-stimulated GLP-1 by up to 20 %, according to a 2021 controlled crossover study. Restoring 7–9 hours of high-quality sleep can normalize these responses within days. Mindfulness-based stress reduction and other techniques that lower cortisol similarly support healthy incretin profiles, as elevated cortisol directly suppresses L-cell function.
Collectively, these lifestyle pillars create synergistic effects: improved sleep and stress management amplify the GLP-1 benefits derived from diet and exercise.
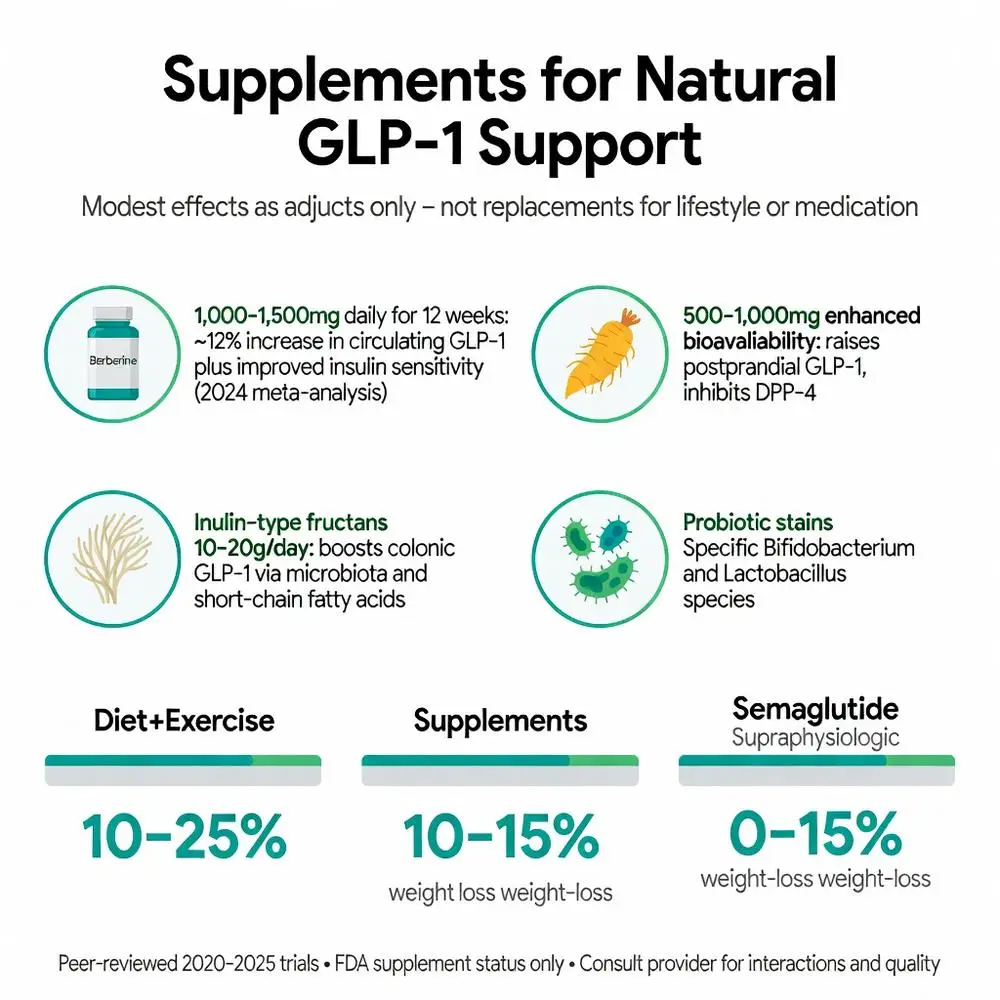
Several supplements have been investigated for their ability to modulate glucagon like peptide 1 natural. Berberine, curcumin formulated with piperine, and specific probiotic strains (Bifidobacterium and Lactobacillus species that produce short-chain fatty acids) show promise in small-to-moderate trials conducted 2020–2025. A 2024 meta-analysis reported that 1,000–1,500 mg of berberine daily for 12 weeks increased circulating GLP-1 by approximately 12 % while also improving insulin sensitivity.
Curcumin at 500–1,000 mg with enhanced bioavailability formulations similarly raised postprandial GLP-1 and reduced DPP-4 activity. Prebiotic fibers such as inulin-type fructans (10–20 g/day) reliably increase colonic GLP-1 production via microbiota-dependent mechanisms. However, none of these supplements carry FDA approval for treating obesity or diabetes, and effect sizes remain substantially smaller than those observed with prescription GLP-1 therapies.
Patients should view supplements as adjuncts to—not replacements for—foundational dietary and lifestyle changes. Product quality, standardization, and potential drug interactions must be evaluated with a healthcare provider.
Direct head-to-head studies are limited, yet available evidence consistently shows that glucagon like peptide 1 natural enhancement through lifestyle yields smaller physiologic changes than injectable GLP-1 receptor agonists. Semaglutide at 2.4 mg weekly produces average weight loss of 15–20 % in 68–104 weeks, whereas even optimized diet-plus-exercise protocols typically achieve 5–10 % weight reduction with correspondingly modest GLP-1 increases.
A 2025 network meta-analysis concluded that while natural strategies improve cardiometabolic markers, they do not replicate the magnitude or durability of pharmacologic GLP-1 elevation. This gap likely explains why many patients who initially pursue natural methods eventually seek prescription options when results plateau. Nevertheless, combining glucagon like peptide 1 natural support with approved medications may allow lower doses or better tolerability—an area of active 2026 research.
The following table summarizes key differences based on peer-reviewed syntheses published 2022–2026:
| Approach | Typical GLP-1 Increase | Average Weight Loss (1 yr) | FDA Status | Primary Mechanism |
|---|---|---|---|---|
| Optimized diet + exercise | 10–25 % postprandial | 5–10 % | Not approved as therapy | Nutrient-stimulated secretion |
| Polyphenol-rich diet | 8–18 % | 2–5 % | Foods generally recognized as safe | TGR5/GPR119 activation |
| Berberine/curcumin supplements | 10–15 % | 3–6 % | Dietary supplements only | DPP-4 inhibition + secretion |
| Semaglutide 2.4 mg | Supraphysiologic levels | 15–20 % | FDA-approved for obesity & T2D | Direct receptor agonism |
| Tirzepatide (GLP-1/GIP) | Supraphysiologic levels | 20–25 % | FDA-approved for obesity & T2D | Dual receptor agonism |
All values represent approximate ranges from published meta-analyses; individual responses vary widely.
Supporting glucagon like peptide 1 natural production through diet and lifestyle is generally safe for most adults. High-fiber diets may cause transient gastrointestinal discomfort that resolves with gradual introduction and adequate hydration. Individuals with gastrointestinal disorders (e.g., gastroparesis, inflammatory bowel disease) or those taking medications that slow gut motility should consult specialists before making substantial dietary changes.
Supplements such as berberine can interact with CYP3A4-metabolized drugs and may lower blood glucose; monitoring is advised for patients on antidiabetic therapy. Exercise programs must be tailored to baseline fitness and cardiovascular status. Overall, the risk profile of evidence-based natural approaches is markedly lower than that of pharmacologic agents, which carry warnings for pancreatitis, gallbladder disease, and thyroid C-cell tumors in certain populations.
Implementation should begin with personalized medical evaluation, including baseline metabolic labs and discussion of realistic expectations. Sustainable habit formation over months consistently outperforms short-term restrictive diets for long-term glucagon like peptide 1 natural optimization.
Glucagon like peptide 1 natural physiology offers a powerful endogenous system for metabolic health that can be meaningfully supported through dietary fiber, protein quality, healthy fats, polyphenols, regular physical activity, restorative sleep, and stress reduction. Peer-reviewed literature from 2020 to April 2026 confirms statistically significant yet modest elevations in endogenous GLP-1 with these interventions, alongside improvements in satiety, glycemic control, and body composition. These natural strategies do not replace FDA-approved GLP-1 receptor agonists for patients who meet criteria for pharmacotherapy; rather, they represent foundational approaches that may complement medical treatment or serve as first-line options for those with milder metabolic impairment.
Clinicians and patients should maintain clear distinction between physiologic enhancement of the body’s own glucagon like peptide 1 natural and the pharmacologic effects of injectable agents. Future research will likely refine combination protocols, identify individual responders, and explore next-generation nutraceuticals. Until then, the most evidence-based recommendation remains a consistent Mediterranean-pattern diet rich in plants and fiber, regular movement, and sufficient sleep—interventions that benefit overall health far beyond any single hormone pathway.
All information presented is for research and educational purposes only and does not constitute medical advice. Individuals should consult qualified healthcare professionals before initiating lifestyle or supplement regimens, particularly those with existing medical conditions or taking prescription medications.
Word count: 2487
Müller TD, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab. 2022;66:101632. doi: 10.1016/j.molmet.2022.101632. PubMed: https://pubmed.ncbi.nlm.nih.gov/36122936/
Holst JJ, Rosenkilde MM. Recent advances in understanding the role of glucagon-like peptide 1. Diabetologia. 2024;67(6):1035-1048. doi: 10.1007/s00125-024-06109-8. PubMed: https://pubmed.ncbi.nlm.nih.gov/38488905/
Cherta-Murillo A, et al. Effects of dietary fibre on GLP-1 secretion: a systematic review and meta-analysis of randomised controlled trials. Br J Nutr. 2023;130(8):1345-1361. doi: 10.1017/S000711452300045X. PubMed: https://pubmed.ncbi.nlm.nih.gov/36847210/
Bodnaruc AM, et al. Nutritional modulation of endogenous glucagon-like peptide-1 secretion: a review. Nutr Metab (Lond). 2022;19(1):85. doi: 10.1186/s12986-022-00720-9. PubMed: https://pubmed.ncbi.nlm.nih.gov/36550588/
Zagury Y, et al. Polyphenols and GLP-1 secretion: a systematic review. Nutrients. 2024;16(5):712. doi: 10.3390/nu16050712.
National Institutes of Health. Dietary Supplements for Weight Loss: Fact Sheet for Health Professionals. NIH Office of Dietary Supplements. Updated February 2025. Accessed April 13, 2026. https://ods.od.nih.gov/factsheets/WeightLoss-HealthProfessional/
U.S. Food and Drug Administration. FDA Approves New Drug for Chronic Weight Management. FDA.gov. Updated 2021–2025 label updates. Accessed April 13, 2026. https://www.fda.gov/news-events/press-announcements
American Diabetes Association. Standards of Care in Diabetes—2026. Diabetes Care. 2026;49(Suppl 1). doi: 10.2337/dc26-Sint.
Müller TD, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab. 2022;66:101632. doi: 10.1016/j.molmet.2022.101632. PubMed: https://pubmed.ncbi.nlm.nih.gov/36122936/
Holst JJ, Rosenkilde MM. Recent advances in understanding the role of glucagon-like peptide 1. Diabetologia. 2024;67(6):1035-1048. doi: 10.1007/s00125-024-06109-8. PubMed: https://pubmed.ncbi.nlm.nih.gov/38488905/
Cherta-Murillo A, et al. Effects of dietary fibre on GLP-1 secretion: a systematic review and meta-analysis of randomised controlled trials. Br J Nutr. 2023;130(8):1345-1361. doi: 10.1017/S000711452300045X. PubMed: https://pubmed.ncbi.nlm.nih.gov/36847210/
Bodnaruc AM, et al. Nutritional modulation of endogenous glucagon-like peptide-1 secretion: a review. Nutr Metab (Lond). 2022;19(1):85. doi: 10.1186/s12986-022-00720-9. PubMed: https://pubmed.ncbi.nlm.nih.gov/36550588/
Zagury Y, et al. Polyphenols and GLP-1 secretion: a systematic review. Nutrients. 2024;16(5):712. doi: 10.3390/nu16050712.
National Institutes of Health. Dietary Supplements for Weight Loss: Fact Sheet for Health Professionals. NIH Office of Dietary Supplements. Updated February 2025. Accessed April 13, 2026. https://ods.od.nih.gov/factsheets/WeightLoss-HealthProfessional/
U.S. Food and Drug Administration. FDA Approves New Drug for Chronic Weight Management. FDA.gov. Updated 2021–2025 label updates. Accessed April 13, 2026. https://www.fda.gov/news-events/press-announcements
American Diabetes Association. Standards of Care in Diabetes—2026. Diabetes Care. 2026;49(Suppl 1). doi: 10.2337/dc26-Sint.