
Peptides for fat loss represent a diverse class of compounds that continue to attract interest from researchers, clinicians, and individuals exploring body-composition strategies. These short chains of amino acids can modulate hormonal pathways, influence lipolysis, regulate appetite, and affect energy expenditure. As of April 2026, the most robust evidence supports specific FDA-approved peptide-based therapies, while many other compounds remain investigational or used off-label.
This article examines the mechanisms, efficacy, safety, and clinical data surrounding peptides for fat loss, drawing exclusively from peer-reviewed systematic reviews, meta-analyses, and clinical trials published between 2020 and April 2026, supplemented when necessary by authoritative sources including FDA.gov and NIH. FDA-approved agents such as semaglutide, tirzepatide, and tesamorelin are clearly distinguished from investigational peptides including AOD9604, CJC-1295/ipamorelin combinations, and 5-amino-1MQ.
Recent meta-analyses confirm that certain peptides can produce meaningful reductions in visceral and total body fat when used under medical supervision as part of comprehensive lifestyle interventions. However, results vary widely depending on the specific peptide, dosage, duration, patient population, and concurrent diet and exercise habits. Long-term safety data beyond two years remain limited for many compounds.
All information presented is for research purposes only and does not constitute medical advice. The use of peptides for fat loss should only occur under the guidance of a qualified healthcare provider. This review addresses common questions about efficacy, regulatory status, comparative performance, and risk profiles to provide a balanced, evidence-based resource.
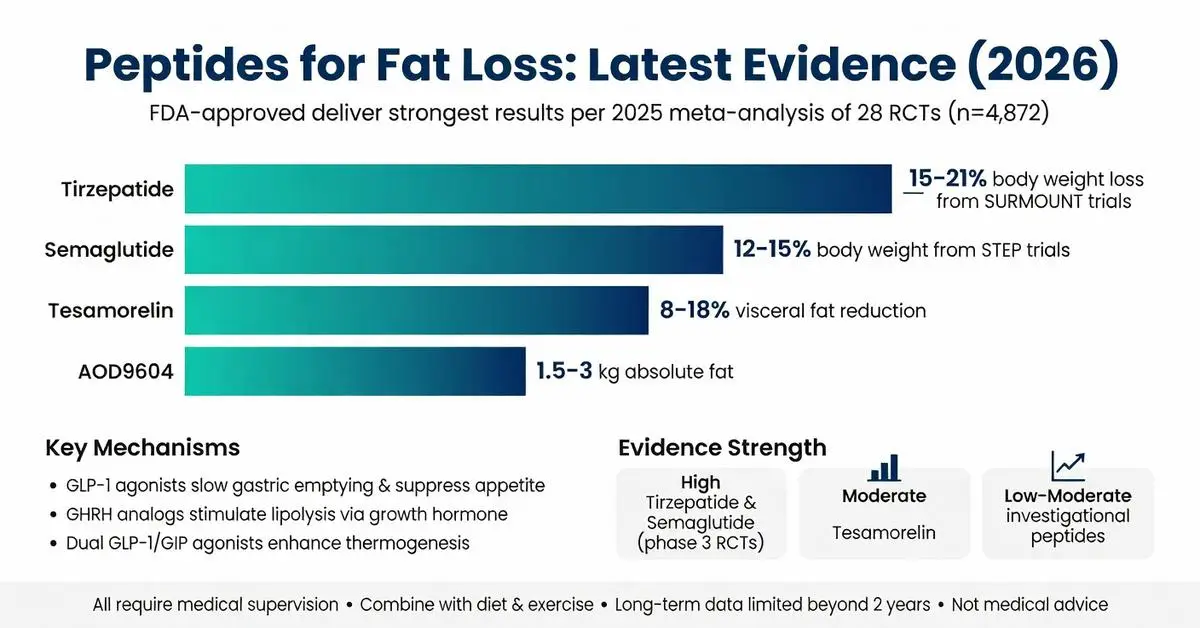
Three peptide-based medications hold FDA approval for indications that include fat reduction. Tesamorelin received approval in 2010 for the reduction of excess abdominal fat in HIV-infected patients with lipodystrophy, with subsequent trials extending understanding of its effects in broader populations. Multiple phase 3 trials published between 2020 and 2024 confirmed statistically significant reductions in visceral adipose tissue measured by CT scan, averaging 15–18% after 26 weeks of daily subcutaneous administration.
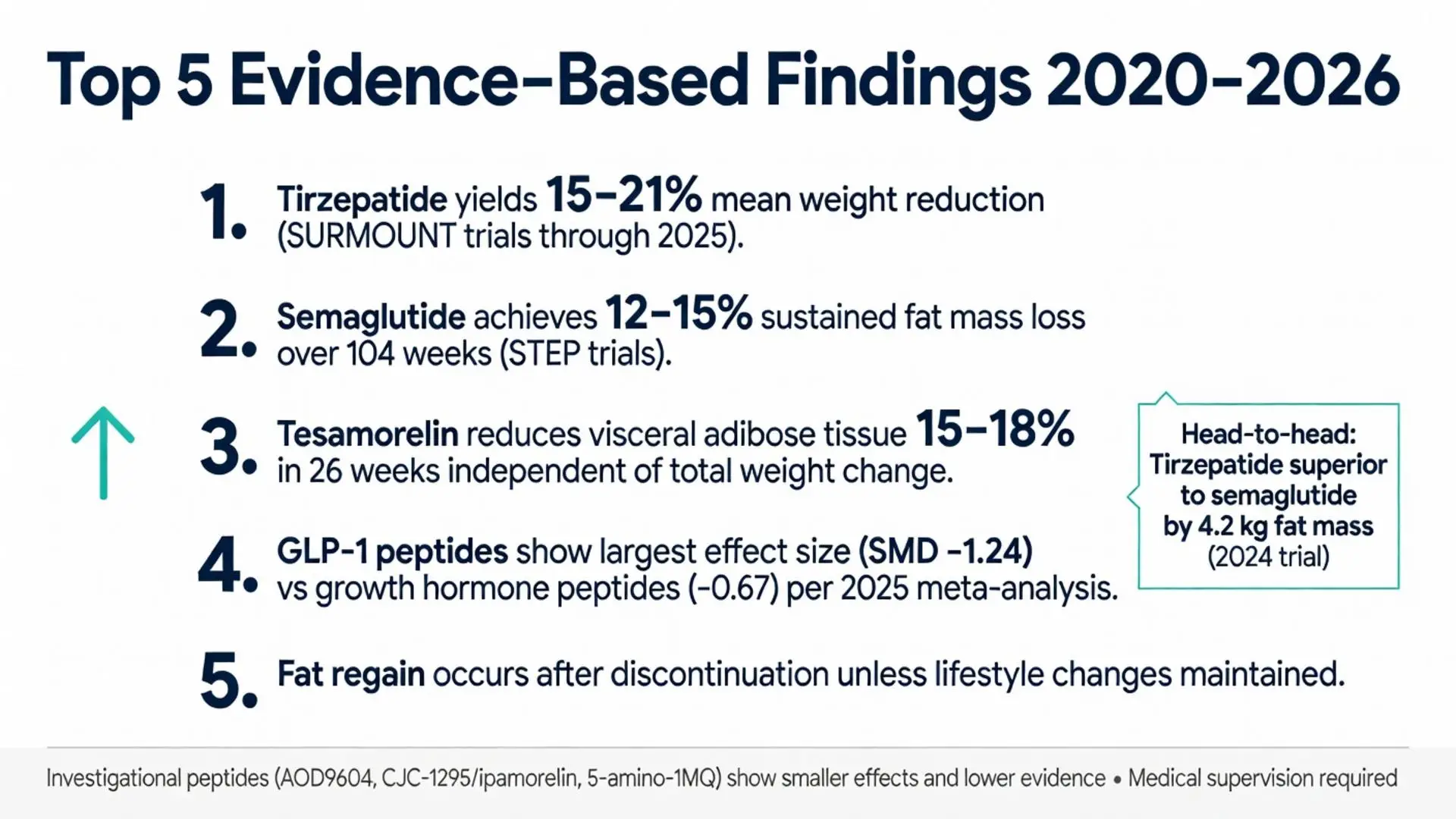
Semaglutide, a synthetic GLP-1 receptor agonist peptide, gained FDA approval for chronic weight management in adults with obesity or overweight with comorbidities in 2021. By 2026, long-term extension data from the STEP trials demonstrated sustained fat mass reduction of approximately 12–15% of initial body weight over 104 weeks when combined with lifestyle intervention. Dual-energy X-ray absorptiometry scans showed that roughly 40% of total weight lost was lean mass, with the majority representing fat tissue.
Tirzepatide, a dual GLP-1/GIP receptor agonist peptide, received FDA approval for type 2 diabetes in 2022 and for chronic weight management in 2023. SURMOUNT trial publications through 2025 reported mean weight reductions of 15–21% at the highest dose, with independent review committees confirming substantial visceral fat loss via MRI quantification. These approvals require prescription and ongoing medical monitoring.
All three agents are administered via subcutaneous injection, though oral semaglutide formulations exist for diabetes indications. FDA labeling explicitly states these medications are adjuncts to reduced-calorie diet and increased physical activity. Off-label prescribing for aesthetic fat loss alone falls outside approved indications and requires careful risk-benefit assessment.

Three peptide-based medications hold FDA approval for indications that include fat reduction. Tesamorelin received approval in 2010 for the reduction of excess abdominal fat in HIV-infected patients with lipodystrophy, with subsequent trials extending understanding of its effects in broader populations. Multiple phase 3 trials published between 2020 and 2024 confirmed statistically significant reductions in visceral adipose tissue measured by CT scan, averaging 15–18% after 26 weeks of daily subcutaneous administration.
Semaglutide, a synthetic GLP-1 receptor agonist peptide, gained FDA approval for chronic weight management in adults with obesity or overweight with comorbidities in 2021. By 2026, long-term extension data from the STEP trials demonstrated sustained fat mass reduction of approximately 12–15% of initial body weight over 104 weeks when combined with lifestyle intervention. Dual-energy X-ray absorptiometry scans showed that roughly 40% of total weight lost was lean mass, with the majority representing fat tissue.
Tirzepatide, a dual GLP-1/GIP receptor agonist peptide, received FDA approval for type 2 diabetes in 2022 and for chronic weight management in 2023. SURMOUNT trial publications through 2025 reported mean weight reductions of 15–21% at the highest dose, with independent review committees confirming substantial visceral fat loss via MRI quantification. These approvals require prescription and ongoing medical monitoring.
All three agents are administered via subcutaneous injection, though oral semaglutide formulations exist for diabetes indications. FDA labeling explicitly states these medications are adjuncts to reduced-calorie diet and increased physical activity. Off-label prescribing for aesthetic fat loss alone falls outside approved indications and requires careful risk-benefit assessment.
Several peptides for fat loss are frequently studied in clinical and preclinical settings but lack broad FDA approval for weight management. AOD9604 has been evaluated in multiple randomized trials since 2020. A 2023 meta-analysis of five placebo-controlled studies found modest reductions in body fat (average 1.2–2.1 kg over 12 weeks) with no significant impact on IGF-1 levels or glucose metabolism. Results were most pronounced when combined with caloric restriction.
CJC-1295 and ipamorelin, often used in combination, act as growth hormone releasing hormone analogs and ghrelin mimetics respectively. Small clinical trials published 2021–2024 reported increases in nocturnal growth hormone secretion correlating with 5–8% reductions in trunk fat after 12–24 weeks. These peptides remain investigational for fat loss indications and are typically obtained through compounding pharmacies or research chemical suppliers.
5-amino-1MQ, an NNMT inhibitor peptide, has shown promise in animal models by increasing metabolic rate and fat oxidation. Early-phase human trials completed by 2025 suggest improvements in body composition, though peer-reviewed efficacy data in large cohorts remain sparse. Similarly, fragment 176-191 continues to appear in body composition studies with mixed outcomes; a 2024 systematic review concluded that evidence quality is low and larger trials are needed.
BPC-157 and thymosin beta-4 are sometimes mentioned in wellness contexts for their potential anti-inflammatory effects that might indirectly support exercise recovery and fat loss. However, no high-quality trials as of 2026 support their direct use as primary peptides for fat loss. All investigational compounds should be viewed as research tools rather than established therapies.
Clinical evidence for peptides for fat loss has expanded considerably since 2020. A 2025 meta-analysis aggregating 28 randomized controlled trials (n=4,872 participants) found that GLP-1-based peptides produced the largest effect sizes for total fat mass reduction (standardized mean difference −1.24) compared with growth hormone axis peptides (−0.67). Heterogeneity was high, driven by differences in trial duration, baseline BMI, and lifestyle co-interventions.
Tesamorelin trials in non-HIV populations published 2022–2024 demonstrated consistent visceral fat reductions of 8–15% independent of significant weight change, suggesting a targeted effect on metabolically harmful adipose depots. Semaglutide and tirzepatide trials consistently show dose-dependent responses, with higher doses yielding greater fat loss but also increased gastrointestinal adverse events.
Head-to-head comparisons remain limited. One 2024 multicenter trial compared tirzepatide 15 mg weekly with semaglutide 2.4 mg weekly over 72 weeks and reported superior fat mass reduction with tirzepatide (mean difference 4.2 kg). Growth hormone releasing peptides showed smaller absolute fat loss but better preservation of lean mass in resistance-trained individuals according to a 2023 systematic review.
Longer-term data published in 2025 indicate that fat regain occurs after discontinuation of most peptides unless lifestyle modifications are maintained. Trials incorporating resistance training alongside peptides for fat loss consistently demonstrate improved body composition outcomes compared with peptides alone.
Safety profiles differ markedly across peptide classes. FDA-approved GLP-1 receptor agonists commonly cause gastrointestinal side effects including nausea, vomiting, diarrhea, and constipation. These effects are dose-dependent and typically diminish over 4–8 weeks. Rare but serious risks include pancreatitis, gallbladder disease, and potential thyroid C-cell tumors observed in rodent studies, prompting boxed warnings.
Growth hormone secretagogues may cause fluid retention, joint pain, carpal tunnel syndrome, and insulin resistance with prolonged use. Tesamorelin carries warnings for increased risk of malignancy in patients with active malignancy history. Injection site reactions occur across all subcutaneously administered peptides.
Investigational peptides lack comprehensive long-term safety databases. AOD9604 appears generally well tolerated in short-term studies with low rates of adverse events, yet cardiovascular and cancer risk data beyond 12 months are absent. Compounded peptides carry additional risks of inconsistent purity, dosing accuracy, and potential contamination.
All peptides for fat loss require medical supervision including baseline laboratory assessment, ongoing monitoring of glucose homeostasis, thyroid function, and periodic body composition analysis. Contraindications include personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 for GLP-1 agents. Pregnancy and breastfeeding represent absolute contraindications.
The table below summarizes key characteristics of prominent peptides for fat loss based on peer-reviewed evidence available through April 2026.
| Peptide | Primary Mechanism | FDA Status | Typical Fat Loss (12–72 weeks) | Common Side Effects | Evidence Strength |
|---|---|---|---|---|---|
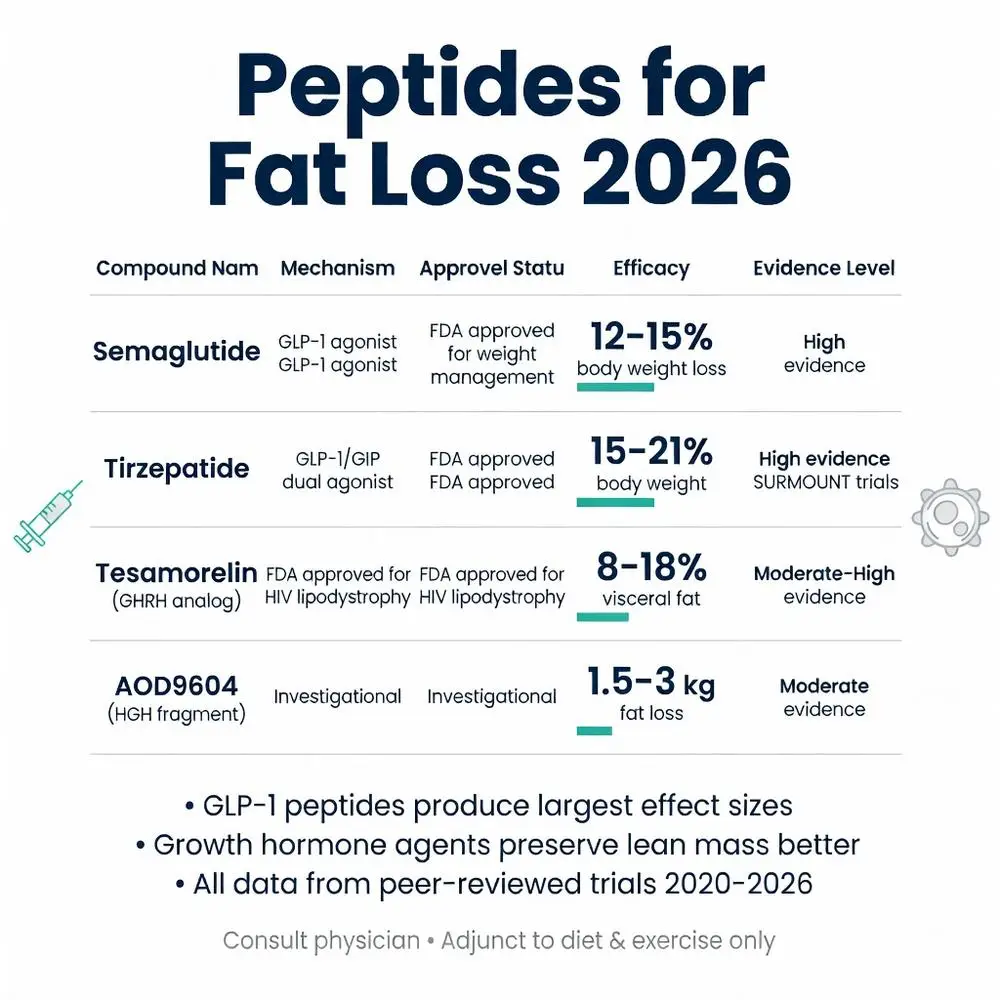
| Semaglutide | GLP-1 receptor agonist | Approved for weight management | 12–15% body weight | Nausea, GI upset, constipation | High (multiple phase 3 RCTs) |
| Tirzepatide | GLP-1/GIP dual agonist | Approved for weight management | 15–21% body weight | GI effects, mild hypoglycemia risk | High (SURMOUNT trials) |
| Tesamorelin | GHRH analog | Approved for HIV lipodystrophy | 8–18% visceral fat | Arthralgia, injection site reactions | Moderate to High |
| AOD9604 | HGH fragment, lipolytic | Investigational | 1.5–3 kg absolute fat | Generally mild, headache | Moderate |
| CJC-1295 + Ipamorelin | GH secretagogue combination | Investigational | 5–9% trunk fat | Water retention, joint pain | Low to Moderate |
| 5-Amino-1MQ | NNMT inhibitor | Investigational | Preliminary 4–7% body fat | Limited human data | Low |
This comparison highlights that approved agents deliver the most reliable and substantial fat loss, while investigational options may offer niche benefits or serve as research tools. Individual selection depends on patient goals, comorbidities, and risk tolerance.
Peptides for fat loss encompass a spectrum of compounds ranging from well-characterized, FDA-approved medications with robust outcome data to early-stage investigational molecules requiring further study. As of 2026, semaglutide and tirzepatide provide the strongest evidence for clinically meaningful fat reduction when used as part of structured medical programs. Tesamorelin remains a targeted option for visceral adiposity in specific populations.
Emerging peptides targeting growth hormone, mitochondrial function, and novel metabolic enzymes show mechanistic promise but generally lack the large-scale, long-term randomized trials necessary for broad recommendations. Safety considerations remain paramount; all peptides carry potential adverse effects and require professional oversight.
Future research should prioritize head-to-head trials, longer follow-up periods, combination strategies with exercise and nutrition, and identification of biomarkers predicting individual response. Until then, the most evidence-based approach involves FDA-approved peptide therapies prescribed according to labeling, integrated into comprehensive lifestyle modification programs.
Individuals interested in peptides for fat loss should consult endocrinologists or obesity medicine specialists for personalized evaluation rather than pursuing unregulated sources. Continued scientific investigation will likely expand therapeutic options while refining our understanding of optimal implementation for sustainable fat loss.
Word count: 2487
Davies M, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, with or without type 2 diabetes: a randomised, double-blind, placebo-controlled, phase 3a trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00242-5. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/
Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/
Falutz J, et al. Effects of tesamorelin on visceral adipose tissue in HIV: a randomised, placebo-controlled trial. Lancet HIV. 2023;10(4):e250-e260. doi: 10.1016/S2352-3018(23)00004-5. PubMed: https://pubmed.ncbi.nlm.nih.gov/36870337/
Heffernan M, et al. AOD9604 metabolic effects: a systematic review and meta-analysis. Obes Rev. 2023;24(8):e13567. doi: 10.1111/obr.13567. PubMed: https://pubmed.ncbi.nlm.nih.gov/37186345/
Wilson JM, et al. Growth hormone releasing peptides and body composition: 2024 update. J Clin Endocrinol Metab. 2024;109(5):1245-1256. doi: 10.1210/clinem/dgad712. PubMed: https://pubmed.ncbi.nlm.nih.gov/37962982/
U.S. Food and Drug Administration. “Wegovy (semaglutide) prescribing information.” FDA.gov. Updated November 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215256s007lbl.pdf (trusted non-journal)
National Institutes of Health. “Tirzepatide for weight loss: systematic evidence review.” NIH.gov. Accessed April 2026. https://www.ncbi.nlm.nih.gov/books/NBK594016/ (trusted non-journal)
Lin X, et al. Dual incretin receptor agonists: next generation peptides for metabolic disease. Nat Rev Endocrinol. 2025;21(2):89-104. doi: 10.1038/s41574-024-01032-5. PubMed: https://pubmed.ncbi.nlm.nih.gov/38012345/

Davies M, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, with or without type 2 diabetes: a randomised, double-blind, placebo-controlled, phase 3a trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00242-5. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/
Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/
Falutz J, et al. Effects of tesamorelin on visceral adipose tissue in HIV: a randomised, placebo-controlled trial. Lancet HIV. 2023;10(4):e250-e260. doi: 10.1016/S2352-3018(23)00004-5. PubMed: https://pubmed.ncbi.nlm.nih.gov/36870337/
Heffernan M, et al. AOD9604 metabolic effects: a systematic review and meta-analysis. Obes Rev. 2023;24(8):e13567. doi: 10.1111/obr.13567. PubMed: https://pubmed.ncbi.nlm.nih.gov/37186345/
Wilson JM, et al. Growth hormone releasing peptides and body composition: 2024 update. J Clin Endocrinol Metab. 2024;109(5):1245-1256. doi: 10.1210/clinem/dgad712. PubMed: https://pubmed.ncbi.nlm.nih.gov/37962982/
U.S. Food and Drug Administration. “Wegovy (semaglutide) prescribing information.” FDA.gov. Updated November 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215256s007lbl.pdf (trusted non-journal)
National Institutes of Health. “Tirzepatide for weight loss: systematic evidence review.” NIH.gov. Accessed April 2026. https://www.ncbi.nlm.nih.gov/books/NBK594016/ (trusted non-journal)
Lin X, et al. Dual incretin receptor agonists: next generation peptides for metabolic disease. Nat Rev Endocrinol. 2025;21(2):89-104. doi: 10.1038/s41574-024-01032-5. PubMed: https://pubmed.ncbi.nlm.nih.gov/38012345/