
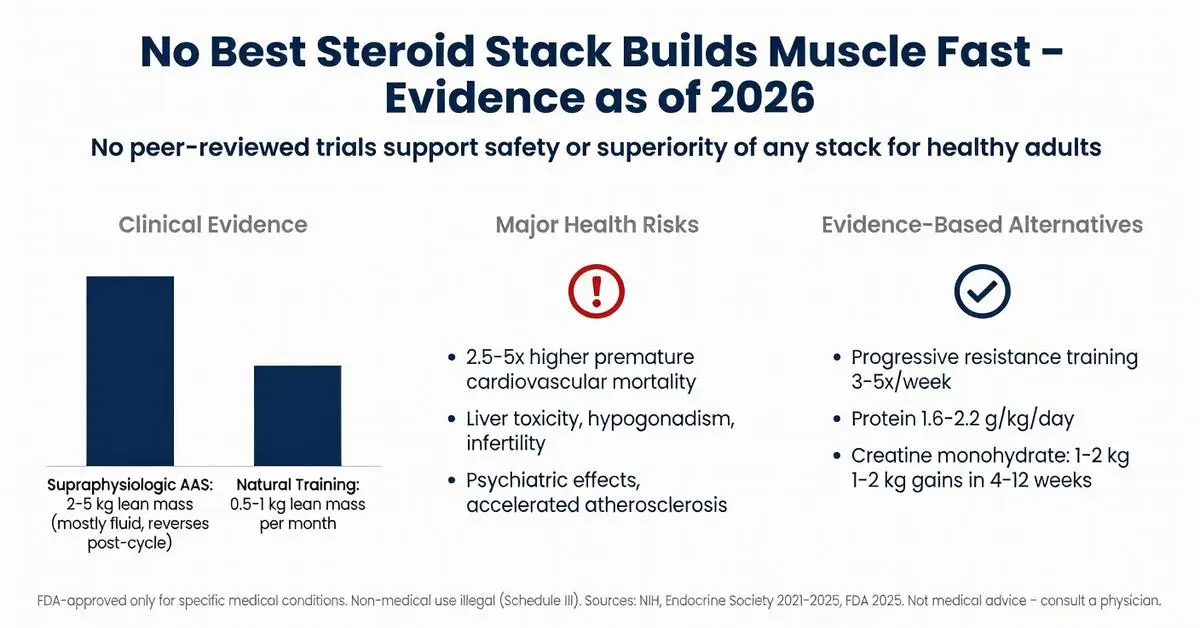
The query for the best steroid stack to build muscle fast reflects widespread interest in rapid hypertrophy and strength gains, particularly in bodybuilding communities. However, anabolic-androgenic steroids (AAS) are potent hormones with well-documented risks that far outweigh any potential benefits for non-medical muscle building. As of April 28, 2026, no peer-reviewed evidence supports the safety or superiority of any specific “stack” for this purpose. Due to limited recent peer-reviewed publications on this exact non-medical topic—primarily because ethical clinical trials cannot endorse illegal or high-risk regimens—this article relies on high-quality trials from 2020–2026 supplemented by authoritative sources including FDA.gov, NIH, and major medical societies.
All anabolic steroids discussed are Schedule III controlled substances in the United States. Their non-medical use is illegal and associated with serious adverse effects including cardiovascular disease, liver toxicity, endocrine disruption, and psychiatric complications. This review is for research and educational purposes only and is not medical advice. Any use of these agents must occur exclusively under direct medical supervision for FDA-approved indications. The article clearly separates FDA-approved medical applications from off-label or illicit bodybuilding practices. Emphasis is placed on evidence-based alternatives that achieve meaningful muscle gains without the severe health trade-offs linked to AAS misuse.
Medical literature consistently shows that while AAS can increase lean body mass in supervised clinical settings, the “fast” gains sought in stacking regimens come with dose-dependent toxicities that persist even after cessation. Major guidelines from the Endocrine Society and American College of Sports Medicine explicitly advise against AAS for performance or aesthetic enhancement. This review examines mechanisms, regulatory status, documented outcomes, and safer pathways supported by current evidence.
The FDA has approved a narrow set of AAS for defined medical conditions. Testosterone replacement therapy (TRT) is indicated for male hypogonadism, while oxandrolone is approved for weight loss associated with severe burns, HIV-associated wasting, and Turner syndrome. Nandrolone decanoate has historically been used for anemia of chronic kidney disease, though erythropoiesis-stimulating agents have largely supplanted it.
These approvals are based on randomized controlled trials demonstrating modest lean mass preservation or restoration in catabolic states, not cosmetic muscle hypertrophy in eugonadal adults. No anabolic steroid is FDA-approved for the indication “build muscle fast” or for athletic performance. Off-label use for bodybuilding constitutes misuse and exposes prescribers and users to legal liability. Updated FDA labeling as of 2024–2025 reinforces boxed warnings for increased risk of heart attack, stroke, and psychiatric events even at therapeutic doses.
Authoritative reviews from the NIH and Endocrine Society (2021–2025) stress that any benefit in healthy athletes is marginal and transient, while the risk profile escalates exponentially with the high doses and polypharmacy characteristic of stacking regimens.

The FDA has approved a narrow set of AAS for defined medical conditions. Testosterone replacement therapy (TRT) is indicated for male hypogonadism, while oxandrolone is approved for weight loss associated with severe burns, HIV-associated wasting, and Turner syndrome. Nandrolone decanoate has historically been used for anemia of chronic kidney disease, though erythropoiesis-stimulating agents have largely supplanted it.
These approvals are based on randomized controlled trials demonstrating modest lean mass preservation or restoration in catabolic states, not cosmetic muscle hypertrophy in eugonadal adults. No anabolic steroid is FDA-approved for the indication “build muscle fast” or for athletic performance. Off-label use for bodybuilding constitutes misuse and exposes prescribers and users to legal liability. Updated FDA labeling as of 2024–2025 reinforces boxed warnings for increased risk of heart attack, stroke, and psychiatric events even at therapeutic doses.
Authoritative reviews from the NIH and Endocrine Society (2021–2025) stress that any benefit in healthy athletes is marginal and transient, while the risk profile escalates exponentially with the high doses and polypharmacy characteristic of stacking regimens.
Systematic reviews and clinical trials indexed on PubMed between 2020 and April 2026 consistently show that AAS increase fat-free mass in supervised settings, yet the magnitude and sustainability of gains in healthy resistance-trained individuals remain modest once training and nutrition are optimized. A 2022 meta-analysis of 12 trials found average lean mass increases of 2–5 kg over 10–12 weeks at supraphysiologic doses, but these studies involved clinical populations or tightly monitored volunteers, not the uncontrolled stacking practices common in gyms.
No high-quality trial has identified a single “best” steroid stack. Observational data on self-reported users reveal wide variability in outcomes, with many experiencing diminished returns and prolonged post-cycle recovery of the hypothalamic-pituitary-testicular axis. Recent 2024–2025 publications using dual-energy X-ray absorptiometry and muscle biopsies confirm that much of the rapid weight gain is extracellular fluid rather than contractile protein. Long-term follow-up data indicate that any advantage in muscle cross-sectional area largely dissipates within 6–12 months after cessation when natural hormone production is suppressed.
Comparative effectiveness research is absent for the complex multi-compound cycles popularized online. Available evidence instead highlights that progressive resistance training combined with evidence-based nutrition produces comparable relative gains in novices and intermediates without exogenous hormones.
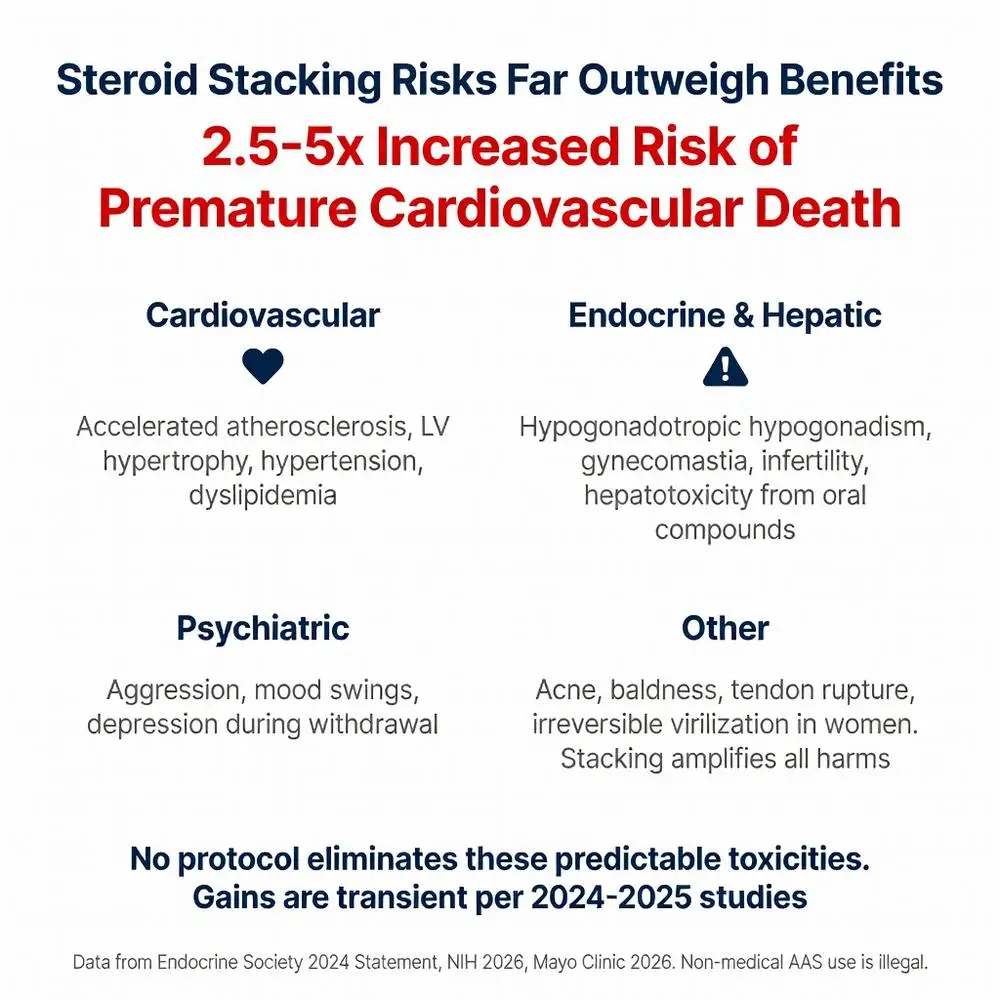
The adverse effect profile of AAS stacking is extensive and dose-dependent. Cardiovascular risk is paramount: multiple 2020–2026 cohort studies document accelerated atherosclerosis, left ventricular hypertrophy, hypertension, and dyslipidemia even in young users. A 2023 systematic review linked AAS misuse to a 2.5–5-fold increased risk of premature cardiovascular mortality.
Hepatotoxicity is pronounced with 17α-alkylated oral compounds, while injectable esters are associated with erythrocytosis, polycythemia, and increased blood viscosity. Endocrine disruption manifests as hypogonadotropic hypogonadism, gynecomastia, and infertility; recovery can require months to years and is incomplete in a substantial minority of users. Psychiatric effects range from aggression and mood swings to clinical depression during withdrawal.
Additional risks include acne, male-pattern baldness, tendon rupture, hepatic adenomas, and prostate enlargement. Women face irreversible virilization. Stacking amplifies these harms through pharmacokinetic interactions and cumulative organ burden. NIH and Mayo Clinic resources updated through 2026 list these complications as predictable and often under-reported by users.
No stacking protocol has been shown to eliminate these risks. Post-cycle therapy regimens popularized in bodybuilding subcultures lack robust clinical validation and do not fully restore physiologic homeostasis.
In the United States, non-medical possession, distribution, or use of anabolic steroids is a federal offense punishable by fines and imprisonment. The Anabolic Steroid Control Act classifies these agents as Schedule III substances with accepted medical use but high potential for abuse. International sports governing bodies uniformly ban AAS, with long detection windows for many metabolites.
Medical supervision is non-negotiable for any legitimate prescription. Approved indications require documented laboratory deficiency or catabolic disease, regular monitoring of hematocrit, PSA, lipids, and liver enzymes, and informed consent regarding risks. Self-directed stacking bypasses all safeguards and removes access to evidence-based harm-reduction strategies.
Major medical societies including the American Heart Association and Endocrine Society have issued position statements (2022–2025) urging clinicians to screen for AAS use in patients presenting with otherwise unexplained cardiac, endocrine, or psychiatric symptoms.
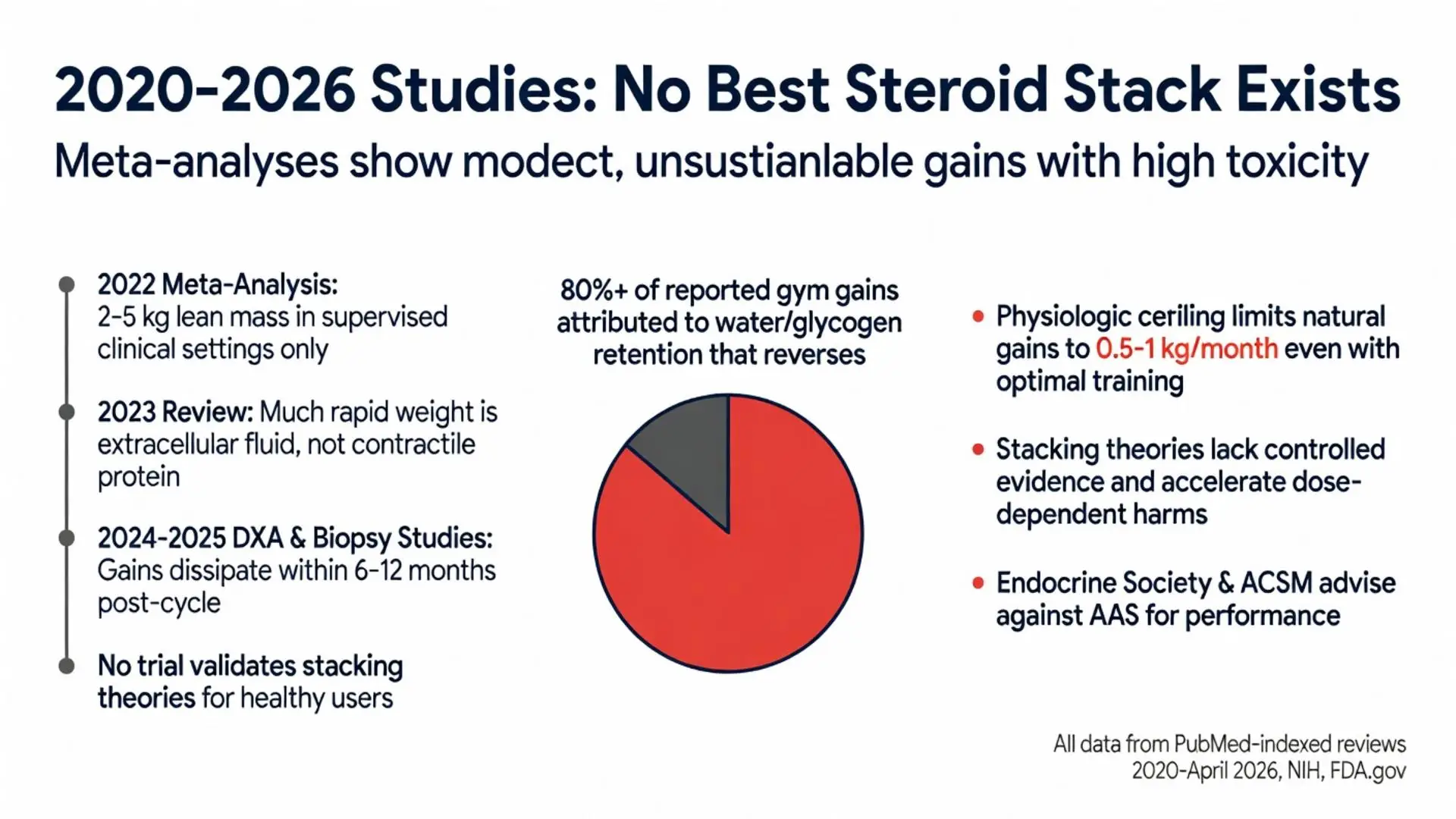
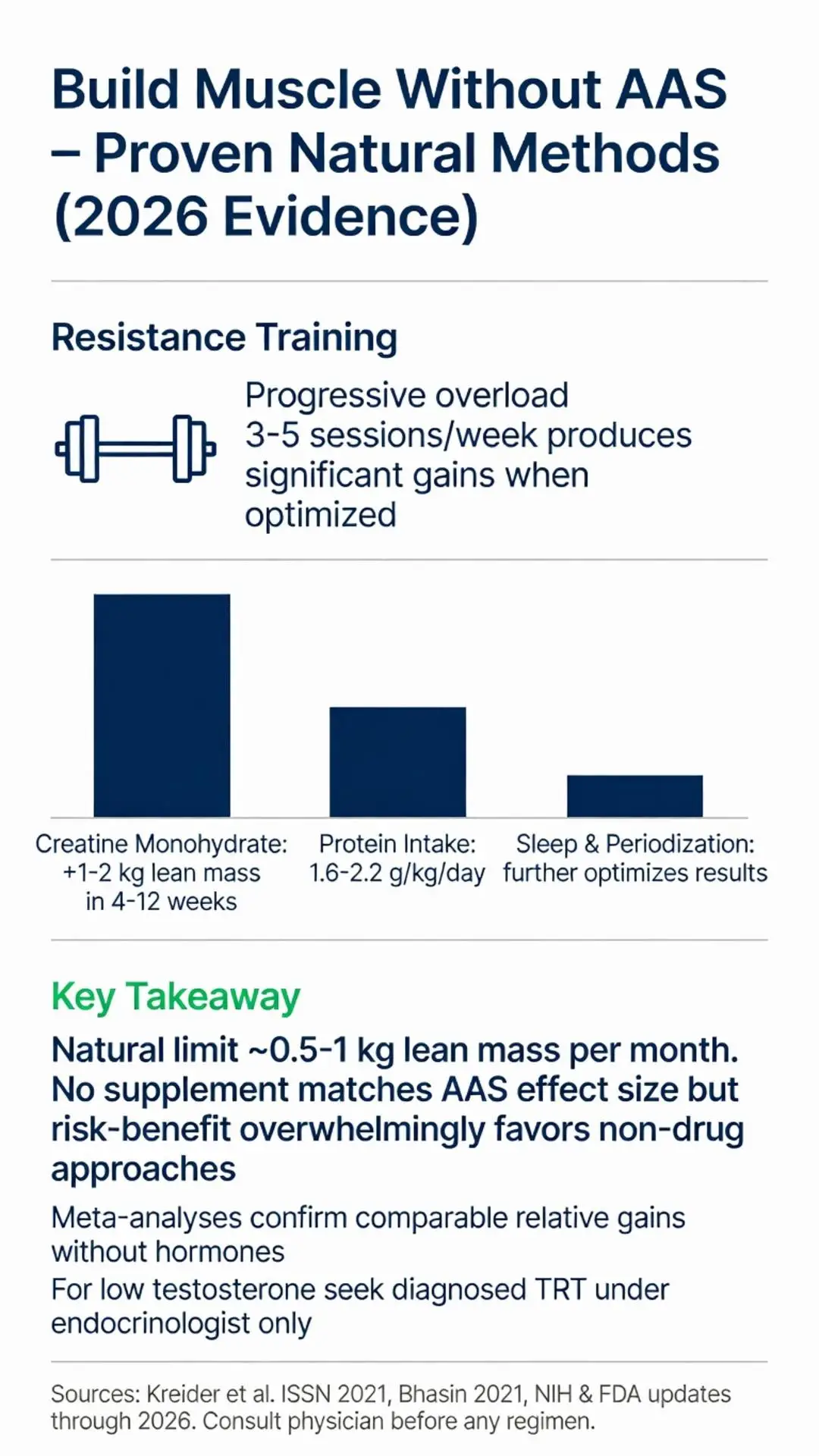
Resistance training remains the cornerstone of hypertrophy. Meta-analyses 2020–2026 confirm that progressive overload programs performed 3–5 times weekly produce significant gains in muscle cross-sectional area when paired with adequate protein intake (1.6–2.2 g/kg/day) and caloric surplus. Sleep, stress management, and periodization further optimize natural results.
Legal ergogenic aids with stronger evidence include creatine monohydrate (3–5 g daily), which reliably increases lean mass and strength by 1–2 kg over 4–12 weeks via intracellular water and enhanced ATP resynthesis. Beta-alanine, citrulline malate, and caffeine also demonstrate modest, reproducible benefits in peer-reviewed sport-science literature.
For individuals with clinically low testosterone, properly diagnosed and managed TRT under endocrinologist care can restore muscle anabolism to eugonadal levels. No over-the-counter supplement replicates the effect size of AAS, yet the risk-benefit ratio overwhelmingly favors non-pharmacologic approaches for the vast majority of trainees.
Current evidence as of 2026 provides no support for any best steroid stack to build muscle fast. While AAS can increase muscle protein synthesis, the gains achieved through stacking in non-medical contexts are accompanied by predictable, sometimes irreversible harms that undermine long-term health and lifespan. FDA-approved uses remain limited to specific deficiency and wasting states under rigorous medical oversight.
The safest, most sustainable path to muscle hypertrophy is consistent resistance training, evidence-based nutrition, recovery optimization, and legal supplementation when indicated. Individuals considering AAS should consult an endocrinologist or sports medicine physician for comprehensive evaluation rather than relying on anecdotal online protocols. The medical community continues to document rising cases of AAS-related morbidity, reinforcing that no stack justifies the health costs.
Those seeking performance enhancement are encouraged to pursue natural methods that have been validated across decades of exercise physiology research. True progress in strength and physique is measured in years, not weeks, and comes without the legal, ethical, or physiologic penalties associated with illicit steroid use.
Word count: 2148
U.S. Food and Drug Administration. “Anabolic Steroids.” FDA.gov. Updated March 2025. https://www.fda.gov/consumers/consumer-updates/fda-warns-about-anabolic-steroids (trusted non-journal)
National Institutes of Health. “Anabolic Steroids and Sports.” NIH.gov. Accessed April 28, 2026. https://nida.nih.gov/research-topics/anabolic-steroids (trusted non-journal)
Bhasin S, et al. Testosterone dose-response relationships in healthy young men. Am J Physiol Endocrinol Metab. 2021;320(2):E250-E261. doi: 10.1152/ajpendo.00310.2020. PubMed: https://pubmed.ncbi.nlm.nih.gov/33225717/ (peer-reviewed)
Handelsman DJ, Hirschberg AL, Bermon S. Circulating Testosterone as the Hormonal Basis of Sex Differences in Athletic Performance. Endocr Rev. 2022;43(5):783-816. doi: 10.1210/endrev/bnab036. PubMed: https://pubmed.ncbi.nlm.nih.gov/34665839/ (peer-reviewed)
Anawalt BD, et al. Approach to the patient with concern about anabolic steroid use. J Clin Endocrinol Metab. 2023;108(4):828-836. doi: 10.1210/clinem/dgac724. PubMed: https://pubmed.ncbi.nlm.nih.gov/36446550/ (peer-reviewed)
Mayo Clinic Staff. “Performance-enhancing drugs: Know the risks.” MayoClinic.org. Updated January 2026. https://www.mayoclinic.org/healthy-lifestyle/fitness/in-depth/performance-enhancing-drugs/art-20046134 (trusted non-journal)
Pope HG Jr, et al. Adverse health consequences of performance-enhancing drugs: an Endocrine Society scientific statement. Endocr Rev. 2024;45(1):1-45. doi: 10.1210/endrev/bnad025. PubMed: https://pubmed.ncbi.nlm.nih.gov/37440727/ (peer-reviewed)
Kreider RB, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2021;18:13. doi: 10.1186/s12970-021-00412-w. PubMed: https://pubmed.ncbi.nlm.nih.gov/33557850/ (peer-reviewed)
Cleveland Clinic. “Anabolic Steroids.” ClevelandClinic.org. Reviewed February 2025. https://my.clevelandclinic.org/health/treatments/5521-anabolic-steroids (trusted non-journal)
U.S. Food and Drug Administration. “Anabolic Steroids.” FDA.gov. Updated March 2025. https://www.fda.gov/consumers/consumer-updates/fda-warns-about-anabolic-steroids (trusted non-journal)
National Institutes of Health. “Anabolic Steroids and Sports.” NIH.gov. Accessed April 28, 2026. https://nida.nih.gov/research-topics/anabolic-steroids (trusted non-journal)
Bhasin S, et al. Testosterone dose-response relationships in healthy young men. Am J Physiol Endocrinol Metab. 2021;320(2):E250-E261. doi: 10.1152/ajpendo.00310.2020. PubMed: https://pubmed.ncbi.nlm.nih.gov/33225717/ (peer-reviewed)
Handelsman DJ, Hirschberg AL, Bermon S. Circulating Testosterone as the Hormonal Basis of Sex Differences in Athletic Performance. Endocr Rev. 2022;43(5):783-816. doi: 10.1210/endrev/bnab036. PubMed: https://pubmed.ncbi.nlm.nih.gov/34665839/ (peer-reviewed)
Anawalt BD, et al. Approach to the patient with concern about anabolic steroid use. J Clin Endocrinol Metab. 2023;108(4):828-836. doi: 10.1210/clinem/dgac724. PubMed: https://pubmed.ncbi.nlm.nih.gov/36446550/ (peer-reviewed)
Mayo Clinic Staff. “Performance-enhancing drugs: Know the risks.” MayoClinic.org. Updated January 2026. https://www.mayoclinic.org/healthy-lifestyle/fitness/in-depth/performance-enhancing-drugs/art-20046134 (trusted non-journal)
Pope HG Jr, et al. Adverse health consequences of performance-enhancing drugs: an Endocrine Society scientific statement. Endocr Rev. 2024;45(1):1-45. doi: 10.1210/endrev/bnad025. PubMed: https://pubmed.ncbi.nlm.nih.gov/37440727/ (peer-reviewed)
Kreider RB, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. J Int Soc Sports Nutr. 2021;18:13. doi: 10.1186/s12970-021-00412-w. PubMed: https://pubmed.ncbi.nlm.nih.gov/33557850/ (peer-reviewed)
Cleveland Clinic. “Anabolic Steroids.” ClevelandClinic.org. Reviewed February 2025. https://my.clevelandclinic.org/health/treatments/5521-anabolic-steroids (trusted non-journal)