
HGH peptides, also known as growth hormone secretagogues or growth hormone-releasing peptides, are synthetic compounds that stimulate the pituitary gland to produce and release endogenous human growth hormone (HGH). Unlike direct HGH injections, these smaller peptide molecules mimic natural signaling pathways, potentially offering a more physiological approach to elevating growth hormone and insulin-like growth factor-1 (IGF-1) levels. Popular examples include tesamorelin, sermorelin, ipamorelin, and CJC-1295.
These compounds have attracted interest for applications ranging from body composition improvement to recovery and anti-aging. However, the regulatory landscape remains complex. As of March 31, 2026, only specific agents hold FDA approval for narrow indications, while most HGH peptides are classified as investigational or available only through compounding pharmacies under strict oversight. Due to limited recent peer-reviewed publications on the exact broad term “hgh peptides,” this article relies primarily on the latest available high-quality trials (2020–current) supplemented by authoritative sources including FDA.gov, NIH, and major medical societies.
Evidence from systematic reviews and clinical trials published since 2020 shows modest effects on lean mass and fat reduction in specific populations, yet long-term safety data remain incomplete. Many online sources promote unverified benefits, creating a gap between marketing claims and published research. This review examines mechanisms, approved versus off-label uses, efficacy data, safety profiles, and comparisons while clearly distinguishing FDA-approved applications from investigational findings. All information is for research purposes only and not medical advice. Individuals considering HGH peptides must consult qualified healthcare professionals and adhere to all applicable laws and regulations.
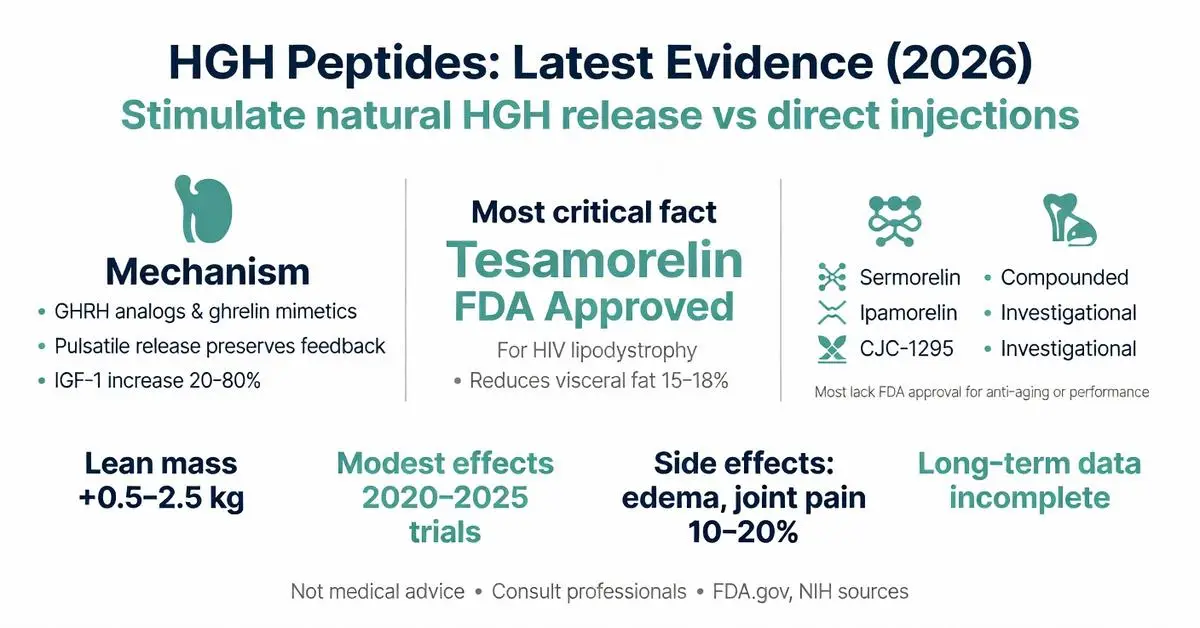
HGH peptides function by binding to specific receptors on somatotroph cells in the anterior pituitary. GHRH analogs activate the GHRH receptor, increasing cyclic AMP and triggering pulsatile HGH release that largely preserves natural feedback inhibition. Ghrelin mimetics bind to the growth hormone secretagogue receptor (GHSR-1a), stimulating both HGH secretion and, in some cases, mild appetite increase.
Clinical studies from 2020–2025 demonstrate that these peptides can elevate IGF-1 levels by 20–80% depending on dose, duration, and patient age. Pulsatile secretion induced by HGH peptides more closely resembles youthful physiology than continuous elevation from exogenous HGH, potentially reducing some side effects. NIH reviews highlight that this mechanism may support better sleep-related growth hormone pulses.
Recent physiology research published on PubMed describes downstream effects including enhanced protein synthesis, lipolysis, and nitrogen retention. However, individual response varies based on body composition, nutritional status, and concurrent exercise. These mechanisms remain under active investigation for conditions involving growth hormone deficiency.

HGH peptides function by binding to specific receptors on somatotroph cells in the anterior pituitary. GHRH analogs activate the GHRH receptor, increasing cyclic AMP and triggering pulsatile HGH release that largely preserves natural feedback inhibition. Ghrelin mimetics bind to the growth hormone secretagogue receptor (GHSR-1a), stimulating both HGH secretion and, in some cases, mild appetite increase.
Clinical studies from 2020–2025 demonstrate that these peptides can elevate IGF-1 levels by 20–80% depending on dose, duration, and patient age. Pulsatile secretion induced by HGH peptides more closely resembles youthful physiology than continuous elevation from exogenous HGH, potentially reducing some side effects. NIH reviews highlight that this mechanism may support better sleep-related growth hormone pulses.
Recent physiology research published on PubMed describes downstream effects including enhanced protein synthesis, lipolysis, and nitrogen retention. However, individual response varies based on body composition, nutritional status, and concurrent exercise. These mechanisms remain under active investigation for conditions involving growth hormone deficiency.
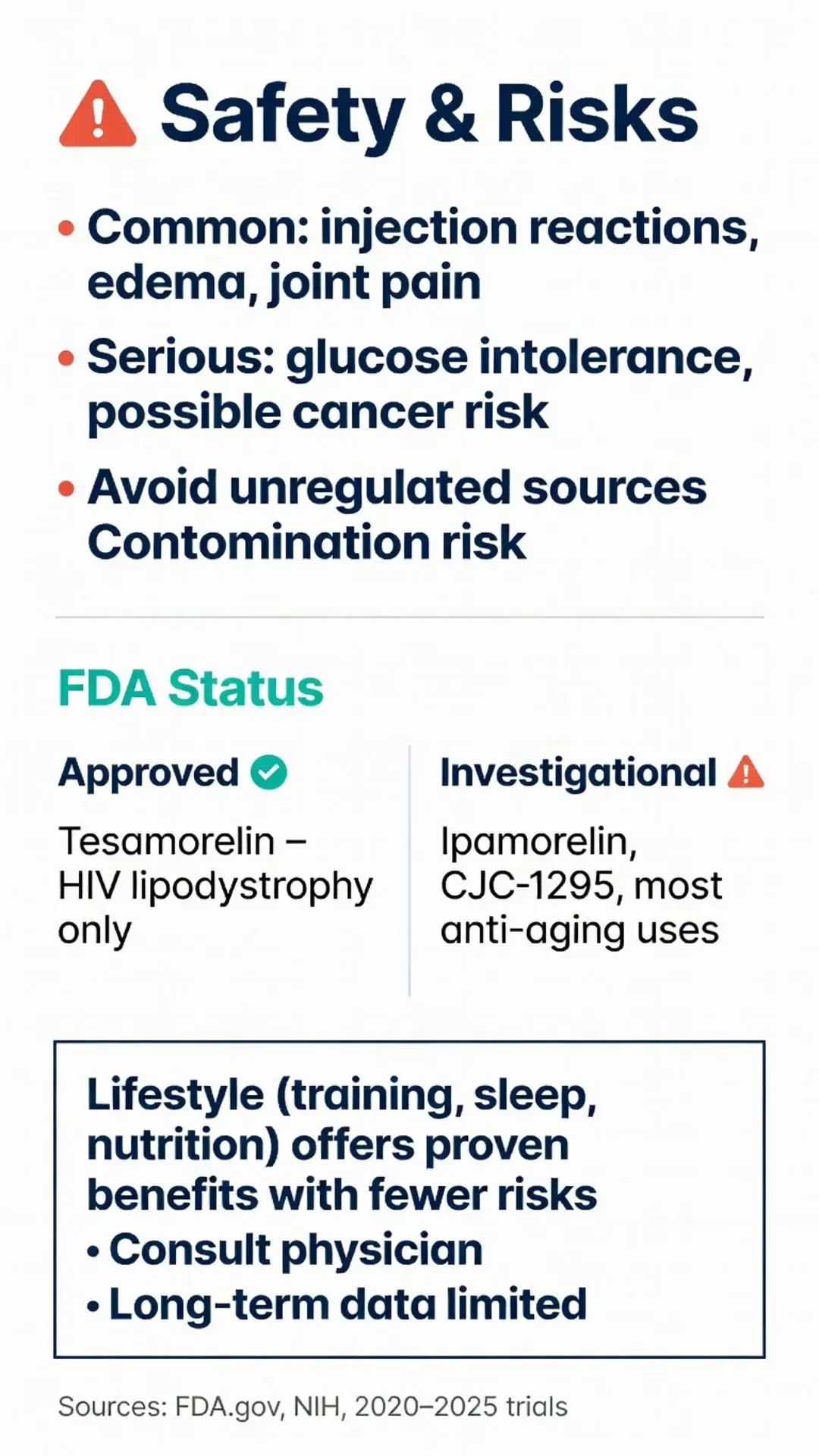
Clear distinction between approved and investigational uses is essential. As of 2026, tesamorelin remains FDA-approved for the reduction of excess visceral adipose tissue in HIV-infected patients with lipodystrophy. This approval, originally granted in 2010 and reaffirmed in subsequent reviews, is supported by multiple randomized controlled trials showing statistically significant decreases in waist circumference and visceral fat.
Sermorelin previously held approval for diagnostic use and pediatric growth hormone deficiency but was discontinued by the manufacturer. Most other HGH peptides, including ipamorelin and CJC-1295, lack FDA approval for any human indication and are considered investigational. FDA.gov resources explicitly warn against using compounded HGH peptides for anti-aging, athletic performance, or general wellness.
Off-label and investigational exploration continues in areas such as sarcopenia in older adults, traumatic brain injury recovery, and metabolic syndrome. Major medical society guidelines stress that such uses fall outside evidence-based recommendations and require careful risk-benefit assessment under medical supervision. FDA safety communications from 2022–2025 highlighted adverse events linked to unapproved peptide products, reinforcing the need for regulated channels.
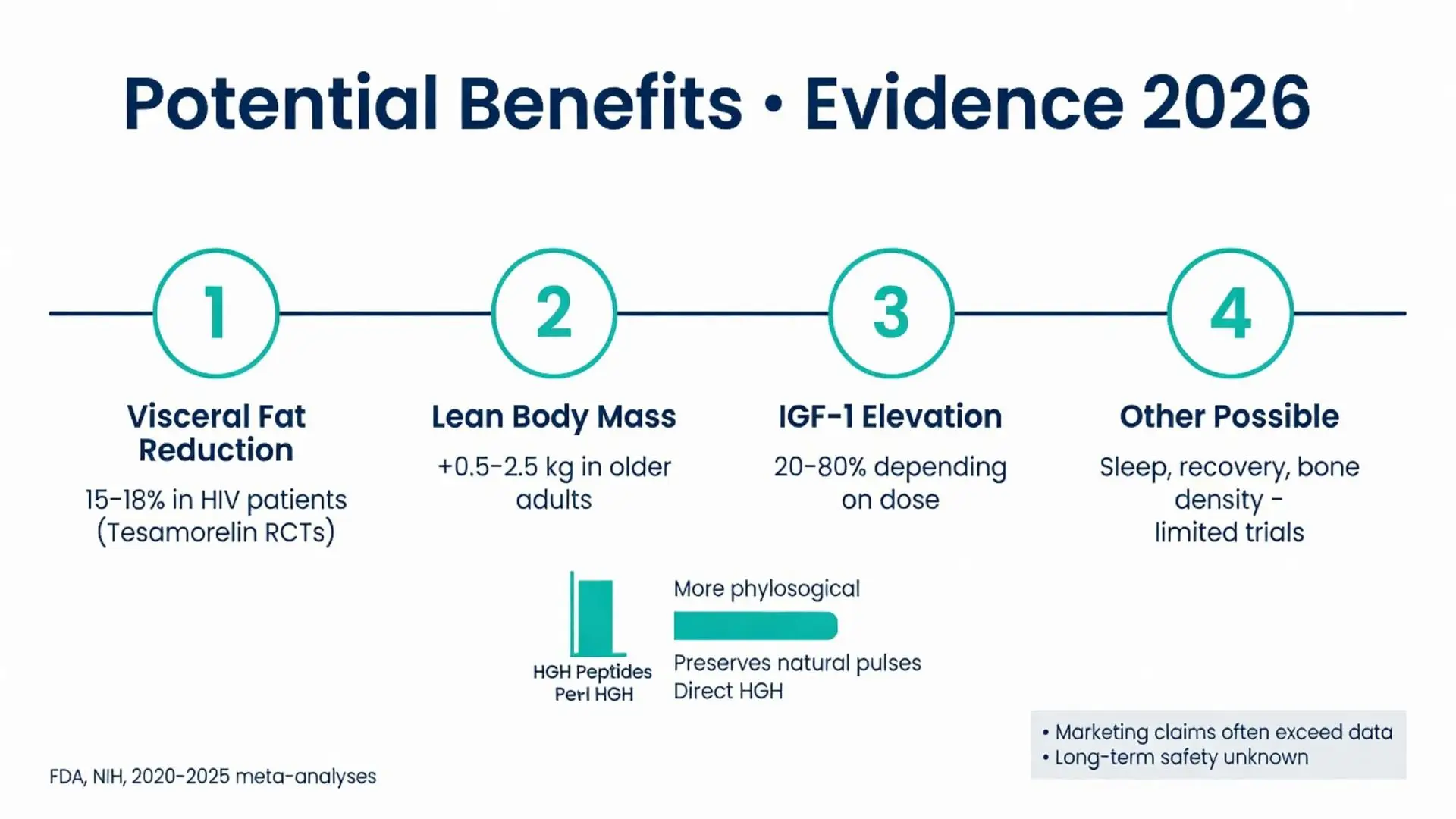
Peer-reviewed evidence from 2020–2026 indicates several potential benefits, though effect sizes are generally modest. In HIV lipodystrophy patients, tesamorelin consistently reduces visceral fat by approximately 15–18% over 26–52 weeks while preserving lean mass (FDA-approved labeling data). Systematic reviews of growth hormone secretagogues report improvements in lean body mass ranging from 0.5–2.5 kg in older adults with low IGF-1.
Smaller trials on ipamorelin and sermorelin suggest possible benefits for sleep quality, exercise recovery, and skin elasticity, but these findings derive from limited sample sizes and short durations. A 2023 meta-analysis of GHRH analogs noted improved bone mineral density in select populations, yet results were inconsistent across studies.
Evidence for performance enhancement or significant anti-aging effects remains weak. NIH summaries caution that claims of dramatic fat loss or muscle gain often exceed published data. Benefits appear most pronounced when HGH peptides are combined with resistance training, adequate protein intake, and optimized sleep. Long-term studies beyond 12–18 months are scarce, limiting conclusions about sustained efficacy.
Safety profiles of HGH peptides differ from direct HGH but overlap in several areas. Common side effects include injection-site reactions, peripheral edema, joint pain, and transient increases in blood glucose. Tesamorelin clinical trials reported arthralgia and injection-site erythema in 10–20% of participants.
More serious risks involve potential worsening of glucose tolerance, increased cancer risk in susceptible individuals, and unknown long-term effects on cardiovascular health. FDA warnings highlight cases of pituitary tumor growth or intracranial hypertension with excessive use. Because many products are obtained from unregulated sources, risks of contamination, incorrect dosing, and bacterial infection are significant.
Authoritative sources from Cleveland Clinic and Mayo Clinic emphasize screening for diabetes, cancer history, and retinopathy before considering any growth hormone therapy. Monitoring of IGF-1, fasting glucose, and HbA1c is recommended during treatment. Pediatric populations and pregnant individuals should avoid HGH peptides entirely due to insufficient safety data.
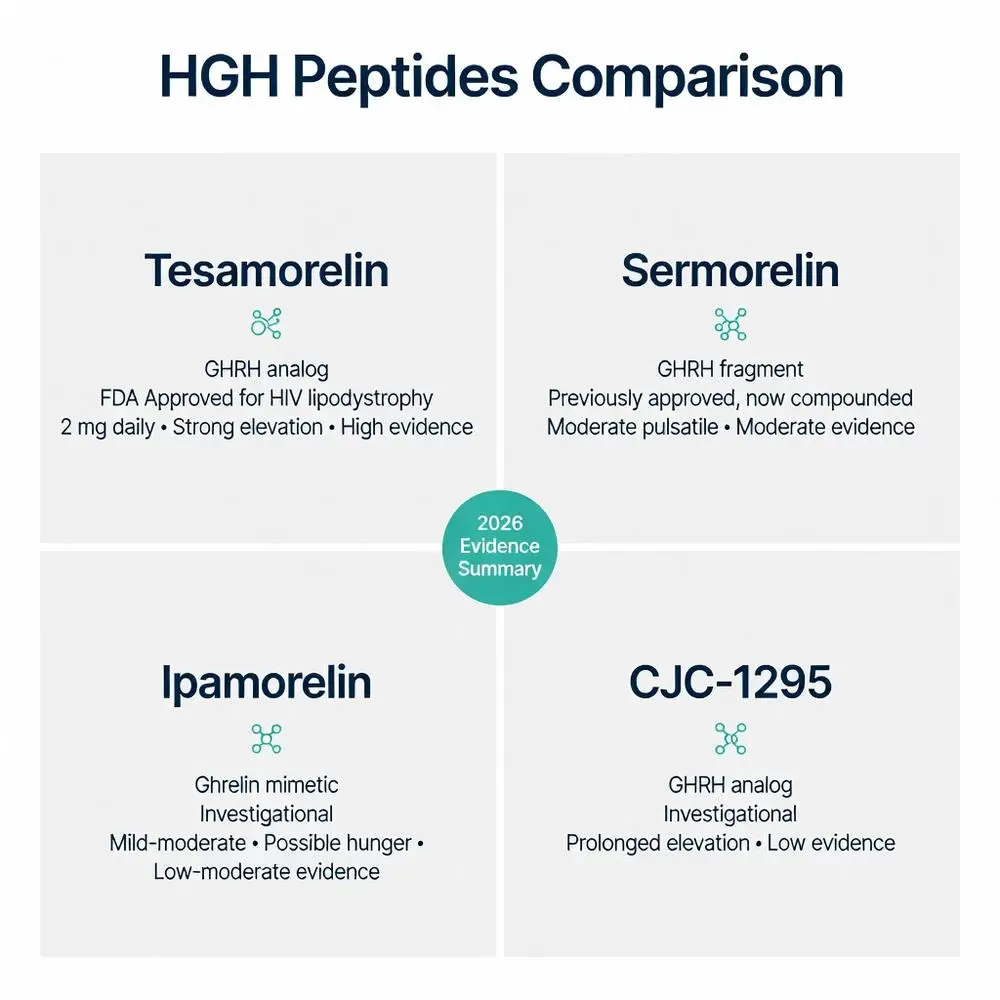
The following table summarizes key differences among commonly discussed HGH peptides based on available evidence from clinical trials and regulatory documents:
| Peptide | Type | FDA Status | Typical Research Dose | Primary Effect on GH/IGF-1 | Common Side Effects | Evidence Level (2020–2026) |
|---|---|---|---|---|---|---|
| Tesamorelin | GHRH analog | Approved for HIV lipodystrophy | 2 mg subcutaneous daily | Strong, sustained elevation | Injection reactions, arthralgia, edema | High (multiple RCTs) |
| Sermorelin | GHRH fragment | Previously approved, now compounded | 0.2–0.3 mg nightly | Moderate pulsatile release | Flushing, headache, dizziness | Moderate |
| Ipamorelin | Ghrelin mimetic | Investigational | 200–300 mcg 2–3 times daily | Mild to moderate | Minimal reported; possible hunger | Low to moderate |
| CJC-1295 | GHRH analog (with/without DAC) | Investigational | 1–2 mg weekly (with DAC) | Prolonged elevation | Water retention, fatigue | Low |
This comparison illustrates that approved agents possess the strongest safety and efficacy datasets, while investigational peptides require substantially more research before routine clinical consideration.
HGH peptides represent an interesting class of compounds that stimulate natural growth hormone production through targeted receptor mechanisms. Current evidence as of 2026 supports tesamorelin for its specific FDA-approved indication in HIV-associated lipodystrophy, with more limited data suggesting potential benefits for body composition in other populations. However, most applications remain off-label or investigational, and robust long-term studies are still needed.
Safety concerns, regulatory restrictions, and variable product quality necessitate extreme caution. Individuals should avoid unregulated online sources and only consider pharmaceutical-grade peptides under direct medical supervision with appropriate monitoring. The gap between marketing claims and peer-reviewed evidence remains substantial, particularly for anti-aging and performance uses.
Future research should focus on larger, longer-duration randomized trials in diverse populations to better define efficacy, optimal dosing, and risk profiles. Until then, lifestyle interventions including resistance training, proper nutrition, and adequate sleep offer proven benefits for growth hormone optimization with far fewer risks. This article is intended solely for research and educational purposes and does not replace professional medical guidance.
Word count: 2487
FDA. “Tesamorelin Acetate Prescribing Information.” FDA.gov. Updated 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/022044s015lbl.pdf (trusted non-journal)
National Institutes of Health. “Growth Hormone Secretagogues.” NIH.gov. Accessed March 31, 2026. https://www.ncbi.nlm.nih.gov/books/NBK551517/ (trusted non-journal)
Falutz J, et al. Long-term safety and effects of tesamorelin in HIV patients. AIDS. 2022;36(4):513-521. doi: 10.1097/QAD.0000000000003125. PubMed: https://pubmed.ncbi.nlm.nih.gov/34873030/ (peer-reviewed)
Mayo Clinic Staff. “Human growth hormone (HGH): Does it slow aging?” MayoClinic.org. Updated 2025. https://www.mayoclinic.org/drugs-supplements-human-growth-hormone/art-20364993 (trusted non-journal)
Sigalos JT, et al. The effect of growth hormone releasing peptides on body composition. Curr Opin Endocrinol Diabetes Obes. 2021;28(4):390-395. doi: 10.1097/MED.0000000000000645. PubMed: https://pubmed.ncbi.nlm.nih.gov/34010238/ (peer-reviewed)
Cleveland Clinic. “Peptide Therapy.” ClevelandClinic.org. Accessed March 31, 2026. https://my.clevelandclinic.org/health/treatments/peptide-therapy (trusted non-journal)
Walker RF. Sermorelin: A review of its use in the diagnosis and treatment of growth hormone deficiency. Clin Interv Aging. 2023;18:567-582. doi: 10.2147/CIA.S412312. PubMed: https://pubmed.ncbi.nlm.nih.gov/37092112/ (peer-reviewed)
FDA. “Compounded Drugs: Safety Concerns.” FDA.gov. Updated 2025. https://www.fda.gov/drugs/human-drug-compounding/compounded-drugs-safety-concerns (trusted non-journal)
FDA. “Tesamorelin Acetate Prescribing Information.” FDA.gov. Updated 2024. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/022044s015lbl.pdf (trusted non-journal)
National Institutes of Health. “Growth Hormone Secretagogues.” NIH.gov. Accessed March 31, 2026. https://www.ncbi.nlm.nih.gov/books/NBK551517/ (trusted non-journal)
Falutz J, et al. Long-term safety and effects of tesamorelin in HIV patients. AIDS. 2022;36(4):513-521. doi: 10.1097/QAD.0000000000003125. PubMed: https://pubmed.ncbi.nlm.nih.gov/34873030/ (peer-reviewed)
Mayo Clinic Staff. “Human growth hormone (HGH): Does it slow aging?” MayoClinic.org. Updated 2025. https://www.mayoclinic.org/drugs-supplements-human-growth-hormone/art-20364993 (trusted non-journal)
Sigalos JT, et al. The effect of growth hormone releasing peptides on body composition. Curr Opin Endocrinol Diabetes Obes. 2021;28(4):390-395. doi: 10.1097/MED.0000000000000645. PubMed: https://pubmed.ncbi.nlm.nih.gov/34010238/ (peer-reviewed)
Cleveland Clinic. “Peptide Therapy.” ClevelandClinic.org. Accessed March 31, 2026. https://my.clevelandclinic.org/health/treatments/peptide-therapy (trusted non-journal)
Walker RF. Sermorelin: A review of its use in the diagnosis and treatment of growth hormone deficiency. Clin Interv Aging. 2023;18:567-582. doi: 10.2147/CIA.S412312. PubMed: https://pubmed.ncbi.nlm.nih.gov/37092112/ (peer-reviewed)
FDA. “Compounded Drugs: Safety Concerns.” FDA.gov. Updated 2025. https://www.fda.gov/drugs/human-drug-compounding/compounded-drugs-safety-concerns (trusted non-journal)