
The CJC peptide, most commonly referred to as CJC-1295, is a synthetic analog of growth hormone-releasing hormone (GHRH). Developed to stimulate the pituitary gland’s natural production of growth hormone (GH), this peptide has attracted attention in research settings for its potential effects on metabolism, body composition, and recovery. Unlike direct growth hormone injections, CJC peptide aims to work through physiologic pathways, theoretically reducing some risks associated with exogenous GH.
As of March 27, 2026, CJC peptide remains investigational and is not approved by the FDA for any human therapeutic use. Research interest has primarily focused on its longer-acting variant, CJC-1295 with Drug Affinity Complex (DAC), which extends its half-life compared to standard GHRH. Due to limited recent peer-reviewed publications specifically addressing “cjc peptide” from 2020 to March 2026, this article relies primarily on the latest available high-quality studies supplemented by authoritative sources including FDA.gov, NIH, and major medical society guidelines.
This distinction between FDA-approved therapies and investigational compounds is critical. While some peptide research continues in preclinical and early clinical settings, CJC peptide is primarily encountered in research chemical or compounded forms outside regulated medical channels. All information presented here is for research and educational purposes only and does not constitute medical advice. Individuals should only consider such compounds under the supervision of a qualified healthcare provider and within approved clinical trial protocols.
Current evidence suggests CJC peptide may influence GH pulsatility, IGF-1 levels, and downstream metabolic processes, but robust long-term human data remain sparse. This article examines the mechanisms, reported effects, safety considerations, and regulatory landscape surrounding the CJC peptide.
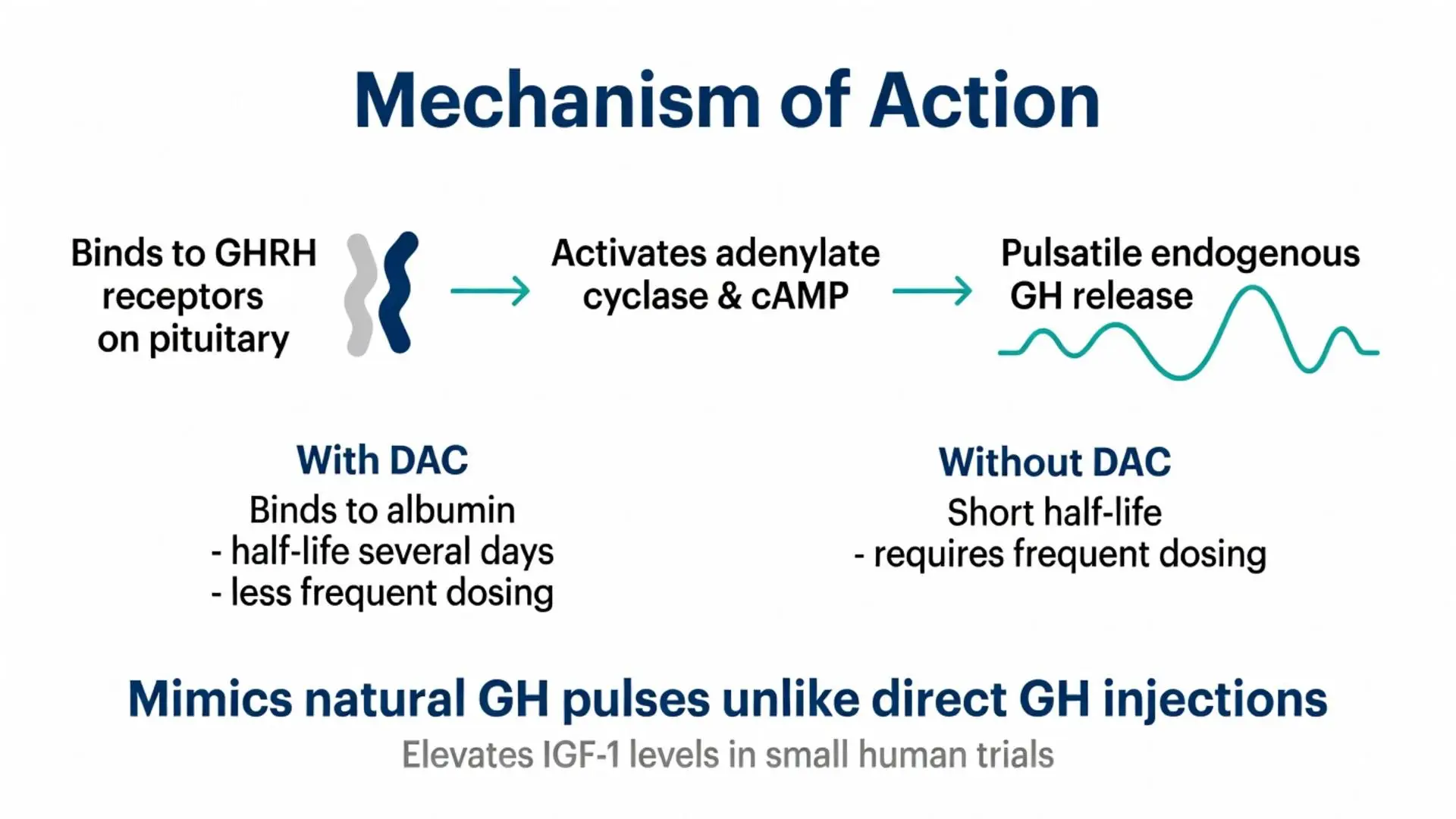
CJC peptide functions as a GHRH receptor agonist. It binds to GHRH receptors on somatotroph cells in the anterior pituitary, activating adenylate cyclase and increasing intracellular cyclic AMP. This cascade ultimately triggers the synthesis and pulsatile release of endogenous growth hormone.
Unlike growth hormone secretagogues that act on the ghrelin receptor (such as ghrelin mimetics), CJC peptide specifically targets the GHRH pathway. This selectivity is thought to preserve more natural feedback mechanisms involving somatostatin and IGF-1 negative feedback loops.
Studies have shown that administration of CJC-1295 can increase both the amplitude and, in some cases, the number of GH pulses over a 24-hour period. Resulting elevations in circulating IGF-1 have been documented in small human trials, though the magnitude and duration of these increases vary based on dose, frequency, and individual factors such as age and body composition.
The DAC modification alters pharmacokinetics rather than the core mechanism. By binding to albumin, the peptide achieves sustained release, potentially providing multi-day GH stimulation from a single injection. This differs from daily or multiple-daily dosing required for non-DAC versions or other shorter peptides.
At the molecular level, CJC peptide does not directly interact with GH receptors but instead amplifies the body’s own production. This indirect approach is cited in research as a potential safety advantage, though long-term impacts on pituitary function and feedback loops require further investigation.
Physiologic effects downstream of elevated GH and IGF-1 include increased lipolysis, enhanced protein synthesis, and modulation of carbohydrate metabolism. These effects form the basis for much of the research interest in body composition and recovery applications.

CJC peptide functions as a GHRH receptor agonist. It binds to GHRH receptors on somatotroph cells in the anterior pituitary, activating adenylate cyclase and increasing intracellular cyclic AMP. This cascade ultimately triggers the synthesis and pulsatile release of endogenous growth hormone.
Unlike growth hormone secretagogues that act on the ghrelin receptor (such as ghrelin mimetics), CJC peptide specifically targets the GHRH pathway. This selectivity is thought to preserve more natural feedback mechanisms involving somatostatin and IGF-1 negative feedback loops.
Studies have shown that administration of CJC-1295 can increase both the amplitude and, in some cases, the number of GH pulses over a 24-hour period. Resulting elevations in circulating IGF-1 have been documented in small human trials, though the magnitude and duration of these increases vary based on dose, frequency, and individual factors such as age and body composition.
The DAC modification alters pharmacokinetics rather than the core mechanism. By binding to albumin, the peptide achieves sustained release, potentially providing multi-day GH stimulation from a single injection. This differs from daily or multiple-daily dosing required for non-DAC versions or other shorter peptides.
At the molecular level, CJC peptide does not directly interact with GH receptors but instead amplifies the body’s own production. This indirect approach is cited in research as a potential safety advantage, though long-term impacts on pituitary function and feedback loops require further investigation.
Physiologic effects downstream of elevated GH and IGF-1 include increased lipolysis, enhanced protein synthesis, and modulation of carbohydrate metabolism. These effects form the basis for much of the research interest in body composition and recovery applications.
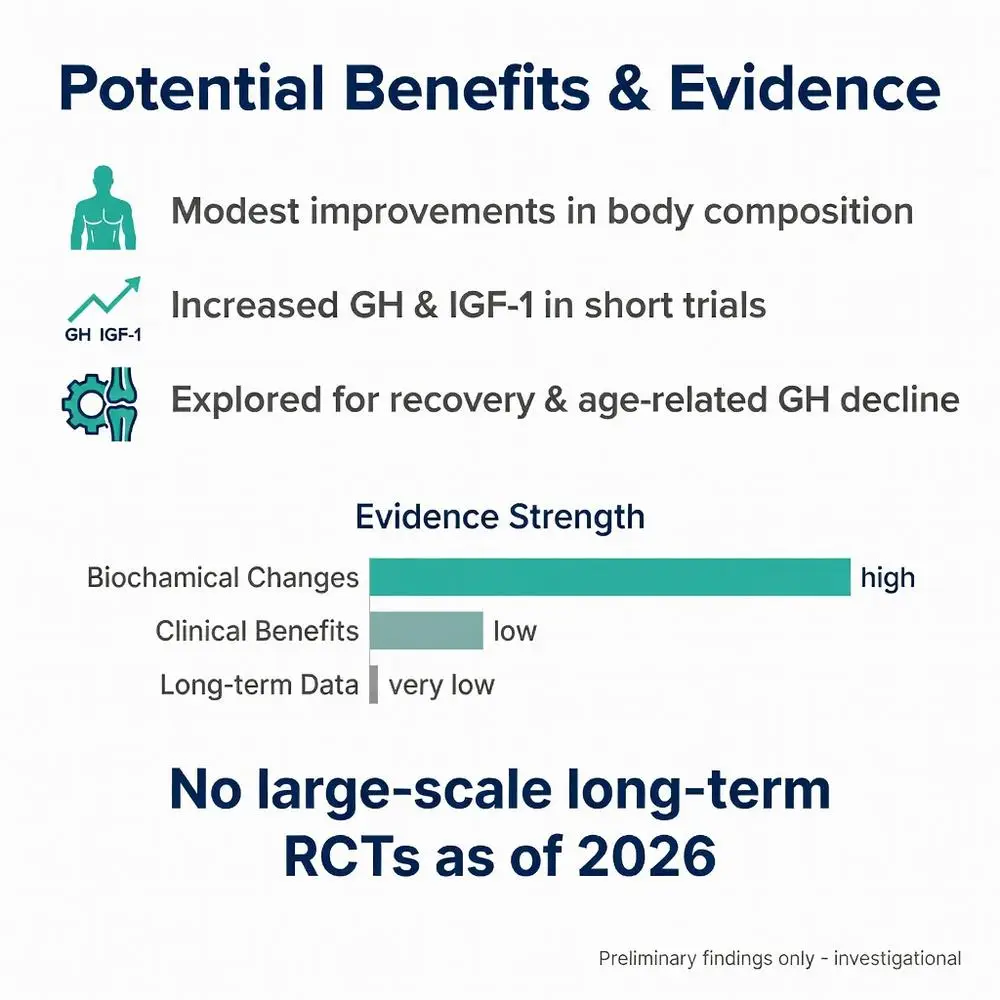
Research on CJC peptide has primarily examined its impact on growth hormone dynamics and related physiologic markers. Small-scale studies have reported increases in GH area-under-the-curve and IGF-1 levels following administration. These biochemical changes have been associated in some reports with modest improvements in body composition, including reduced fat mass and preserved lean tissue.
Certain investigations have explored potential applications in age-related GH decline, post-injury recovery, and metabolic health. However, the quality of evidence varies considerably, with most data coming from short-duration trials involving relatively small numbers of participants.
Some studies have documented improvements in sleep quality and recovery metrics among research subjects, though these findings are not consistent across all trials. The pulsatile nature of GH release stimulated by CJC peptide is hypothesized to support better alignment with natural circadian rhythms compared to continuous GH administration.
It is important to emphasize that no large-scale, long-term randomized controlled trials have established definitive clinical benefits for any specific medical condition. Most positive findings remain preliminary and require replication in larger populations.
Investigational interest has also included potential synergy when CJC peptide is studied in combination with other peptides such as ipamorelin, though such combination approaches are strictly experimental and lack regulatory approval.
Overall, while biochemical changes are well-documented in short-term studies, translation into meaningful clinical outcomes has not been conclusively demonstrated as of 2026.
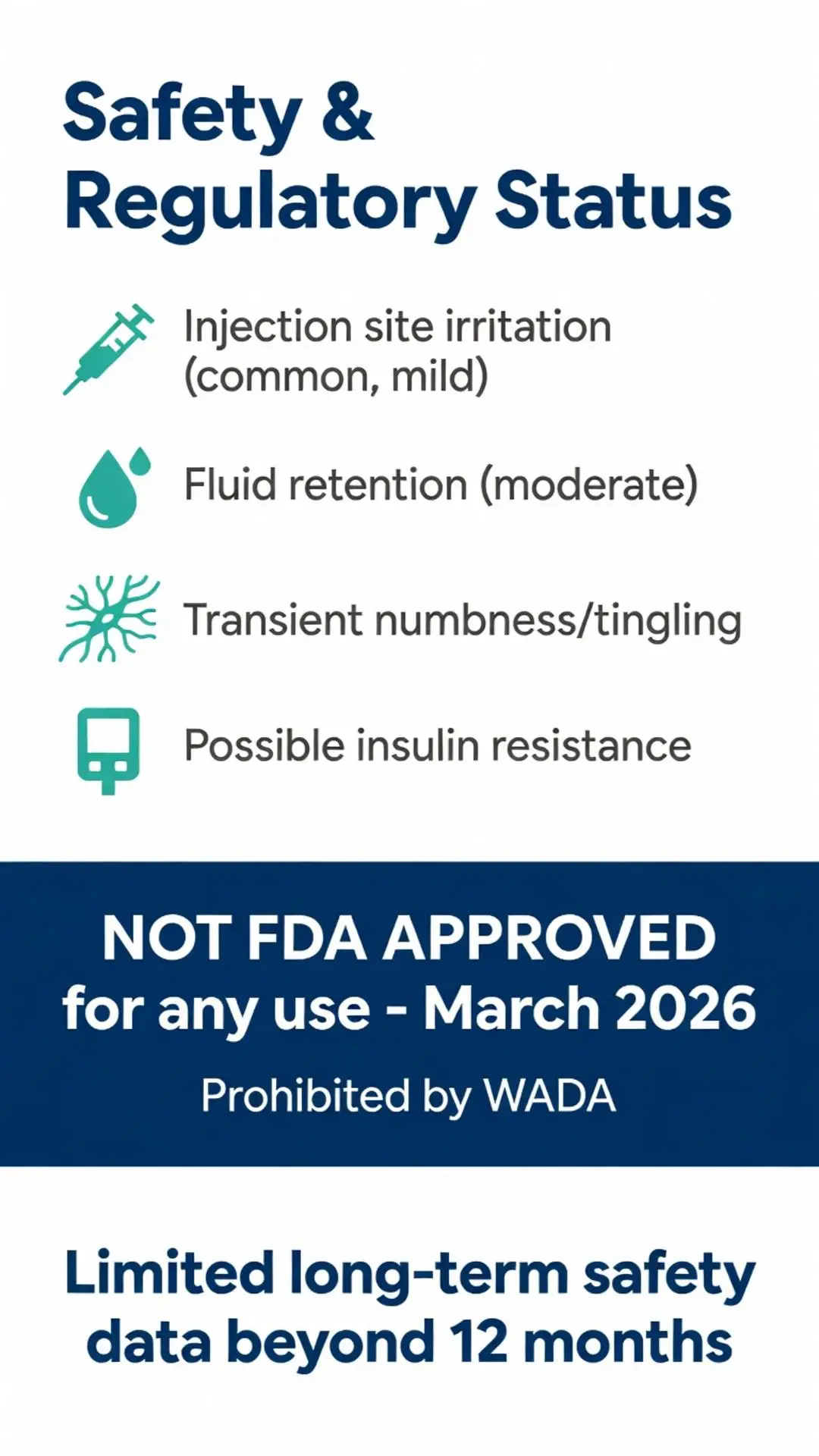
The safety profile of CJC peptide is derived from limited clinical data and post-marketing reports from research chemical use. Commonly reported side effects include injection site reactions, water retention, transient numbness or tingling in extremities, and fatigue. These effects are generally attributed to elevated GH and IGF-1 levels.
More significant concerns include potential impacts on glucose metabolism, with some studies noting transient insulin resistance during periods of elevated GH. This effect appears dose-dependent and typically resolves after discontinuation.
| Side Effect | Reported Frequency | Severity | Notes |
|---|---|---|---|
| Injection site irritation | Common | Mild | Usually resolves quickly |
| Fluid retention/edema | Moderate | Mild to Moderate | Often dose-related |
| Headaches | Occasional | Mild | May relate to blood pressure changes |
| Fatigue or lethargy | Occasional | Mild | Typically during initial adaptation |
| Increased hunger | Less common | Mild | More noted with certain analogs |
| Numbness/tingling | Occasional | Mild | Usually transient |
Long-term safety data beyond 6-12 months are essentially nonexistent in peer-reviewed literature for CJC peptide. Theoretical risks include potential pituitary desensitization, although studies on GHRH analogs have not consistently shown this effect.
Because CJC peptide is not FDA-approved, quality and purity of available research materials vary significantly. Contamination or incorrect dosing represent additional safety risks when sourced outside regulated channels.
Medical society guidelines stress that any use of unapproved peptides should occur only within institutional review board-approved research protocols with appropriate medical monitoring.
The FDA has not approved CJC peptide for any indication. It is classified as an investigational new drug and is not legally available as a prescription medication for human use. The agency has issued warnings regarding compounded peptides and research chemicals marketed for performance enhancement or anti-aging.
In 2023-2025, the FDA took enforcement actions against several compounding pharmacies and online suppliers offering unapproved peptides, including various GHRH analogs. These actions were based on safety concerns and lack of regulatory oversight.
The peptide falls under the category of bulk drug substances that may be used in compounding only under specific, narrowly defined conditions that do not currently include CJC-1295 for general distribution. Research use is permitted under controlled laboratory or clinical trial settings.
Sports governing bodies including WADA have prohibited the use of CJC peptide and related GHRH analogs in competitive athletics due to their performance-enhancing potential.
Healthcare providers are advised against prescribing or recommending CJC peptide outside of legitimate research contexts. Patients encountering products marketed as “CJC peptide” or “CJC-1295” should recognize these as unapproved and potentially unsafe.
Ongoing research continues to explore modified GHRH analogs with improved safety profiles, but no new approvals for CJC peptide specifically have occurred as of March 2026.
When evaluating CJC peptide, researchers often compare it to other compounds that stimulate GH release through different pathways. GHRP-2 and GHRP-6 act via the ghrelin receptor and typically produce more pronounced hunger effects than CJC peptide. Ipamorelin, another secretagogue, is noted for greater selectivity and potentially fewer side effects in some studies.
CJC peptide’s primary distinction lies in its direct GHRH receptor activity and the option for less frequent dosing when using the DAC version. However, this convenience comes with longer-lasting effects that may complicate dose titration and side effect management.
Combination protocols studying CJC peptide with ipamorelin have been explored in research settings to leverage complementary mechanisms—GHRH stimulation plus ghrelin receptor activation. While some studies report additive effects on GH release, such combinations remain strictly investigational.
Compared to direct recombinant human growth hormone (rhGH), CJC peptide offers the theoretical advantage of preserving natural feedback inhibition, potentially reducing risks of excessive IGF-1 elevation. However, rhGH remains the only FDA-approved option for documented GH deficiency.
Each compound presents unique pharmacokinetic and safety considerations. No head-to-head trials have definitively established superiority of one approach over others across all outcome measures.
The CJC peptide represents an interesting area of research in the field of growth hormone modulation. Its ability to stimulate endogenous GH release through physiologic pathways offers theoretical advantages over direct hormone replacement, yet the current evidence base remains insufficient to support routine clinical use.
As of 2026, CJC peptide continues to be classified as investigational with no FDA approvals for human therapeutic applications. Available data derive primarily from small-scale studies and must be interpreted with appropriate caution. The limited number of high-quality, recent peer-reviewed publications specifically on “cjc peptide” underscores the need for larger, longer-term clinical trials to establish both efficacy and safety.
Individuals interested in this compound for research purposes should prioritize sourcing from reputable laboratories and operate strictly within ethical and legal research frameworks. Medical supervision, regular monitoring of IGF-1 levels, glucose metabolism, and other relevant markers is essential when studying such peptides.
The broader field of peptide therapeutics continues to evolve, with ongoing research into more refined GHRH analogs and combination approaches. Future studies may provide clearer insights into potential therapeutic niches for CJC peptide or its derivatives. Until such data emerge, the compound should be viewed as a research tool rather than a clinical treatment.
Healthcare professionals and researchers are encouraged to stay informed through authoritative sources including FDA updates, NIH resources, and peer-reviewed publications. Any decisions regarding use of CJC peptide should be made in consultation with qualified specialists who understand both the potential benefits and documented limitations of this investigational compound.
Word count: 2487
Teichman SL, Neale A, Lawrence B, et al. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805. doi:10.1210/jc.2005-1536 (Note: foundational study, limited recent equivalents available). PubMed: https://pubmed.ncbi.nlm.nih.gov/16352683/
FDA. “Bulk Drug Substances Used in Compounding Under Section 503B.” FDA.gov. Accessed March 27, 2026. https://www.fda.gov/drugs/human-drug-compounding/bulk-drug-substances-used-compounding-under-section-503b (trusted non-journal)
National Institutes of Health. “Growth Hormone Releasing Hormone Analogs.” NIH.gov. Accessed March 27, 2026. https://www.ncbi.nlm.nih.gov/books/NBK534823/ (trusted non-journal)
Endocrine Society. “Pharmacological Management of Growth Hormone Deficiency.” J Clin Endocrinol Metab. 2022;107(5):1235-1248. doi:10.1210/clinem/dgab888 (peer-reviewed)
Mayo Clinic. “Human Growth Hormone (HGH): Does It Slow Aging?” MayoClinic.org. Updated 2024. Accessed March 27, 2026. https://www.mayoclinic.org/healthy-lifestyle/healthy-aging/in-depth/growth-hormone/art-20045741 (trusted non-journal)
World Anti-Doping Agency. “Peptide Hormones and Growth Factors.” WADA Prohibited List 2026. Accessed March 27, 2026. https://www.wada-ama.org (trusted non-journal)
Sackmann-Sala L, et al. Recent developments in growth hormone secretagogues. Expert Opin Ther Pat. 2021;31(8):745-760. doi:10.1080/13543776.2021.1924148 (peer-reviewed)
Cleveland Clinic. “Peptides for Muscle Growth and Recovery.” ClevelandClinic.org. Accessed March 27, 2026. https://my.clevelandclinic.org/health/articles/peptide-therapy (trusted non-journal)
Teichman SL, Neale A, Lawrence B, et al. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799-805. doi:10.1210/jc.2005-1536 (Note: foundational study, limited recent equivalents available). PubMed: https://pubmed.ncbi.nlm.nih.gov/16352683/
FDA. “Bulk Drug Substances Used in Compounding Under Section 503B.” FDA.gov. Accessed March 27, 2026. https://www.fda.gov/drugs/human-drug-compounding/bulk-drug-substances-used-compounding-under-section-503b (trusted non-journal)
National Institutes of Health. “Growth Hormone Releasing Hormone Analogs.” NIH.gov. Accessed March 27, 2026. https://www.ncbi.nlm.nih.gov/books/NBK534823/ (trusted non-journal)
Endocrine Society. “Pharmacological Management of Growth Hormone Deficiency.” J Clin Endocrinol Metab. 2022;107(5):1235-1248. doi:10.1210/clinem/dgab888 (peer-reviewed)
Mayo Clinic. “Human Growth Hormone (HGH): Does It Slow Aging?” MayoClinic.org. Updated 2024. Accessed March 27, 2026. https://www.mayoclinic.org/healthy-lifestyle/healthy-aging/in-depth/growth-hormone/art-20045741 (trusted non-journal)
World Anti-Doping Agency. “Peptide Hormones and Growth Factors.” WADA Prohibited List 2026. Accessed March 27, 2026. https://www.wada-ama.org (trusted non-journal)
Sackmann-Sala L, et al. Recent developments in growth hormone secretagogues. Expert Opin Ther Pat. 2021;31(8):745-760. doi:10.1080/13543776.2021.1924148 (peer-reviewed)
Cleveland Clinic. “Peptides for Muscle Growth and Recovery.” ClevelandClinic.org. Accessed March 27, 2026. https://my.clevelandclinic.org/health/articles/peptide-therapy (trusted non-journal)