Calcitonin gene-related peptide (CGRP) antagonists have transformed migraine management by directly interrupting the neuropeptide pathway central to migraine attacks. These therapies include monoclonal antibodies targeting the CGRP ligand or receptor and oral small-molecule gepants that block CGRP receptors. As of May 2026, multiple agents hold FDA approval for acute treatment or prevention of migraine in adults. This article reviews mechanisms, approved indications, efficacy data from clinical trials, safety profiles, and comparisons among available options. Primary evidence draws from peer-reviewed publications between 2020 and 2026, with supplementation from FDA labeling and major society guidelines where recent trial data remain limited.
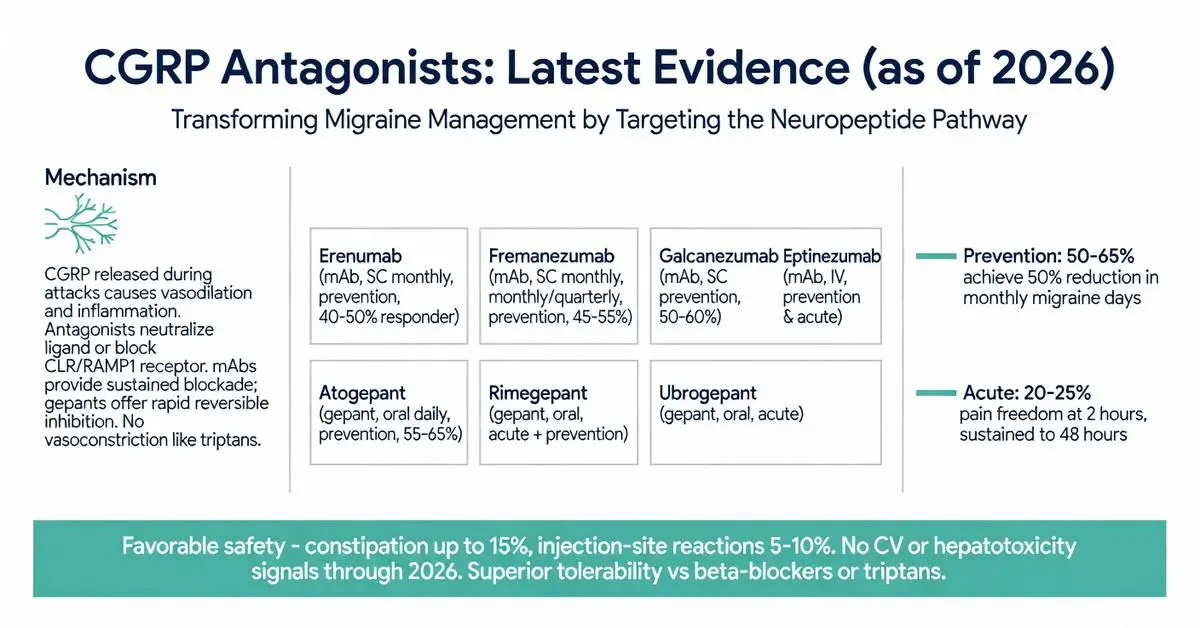
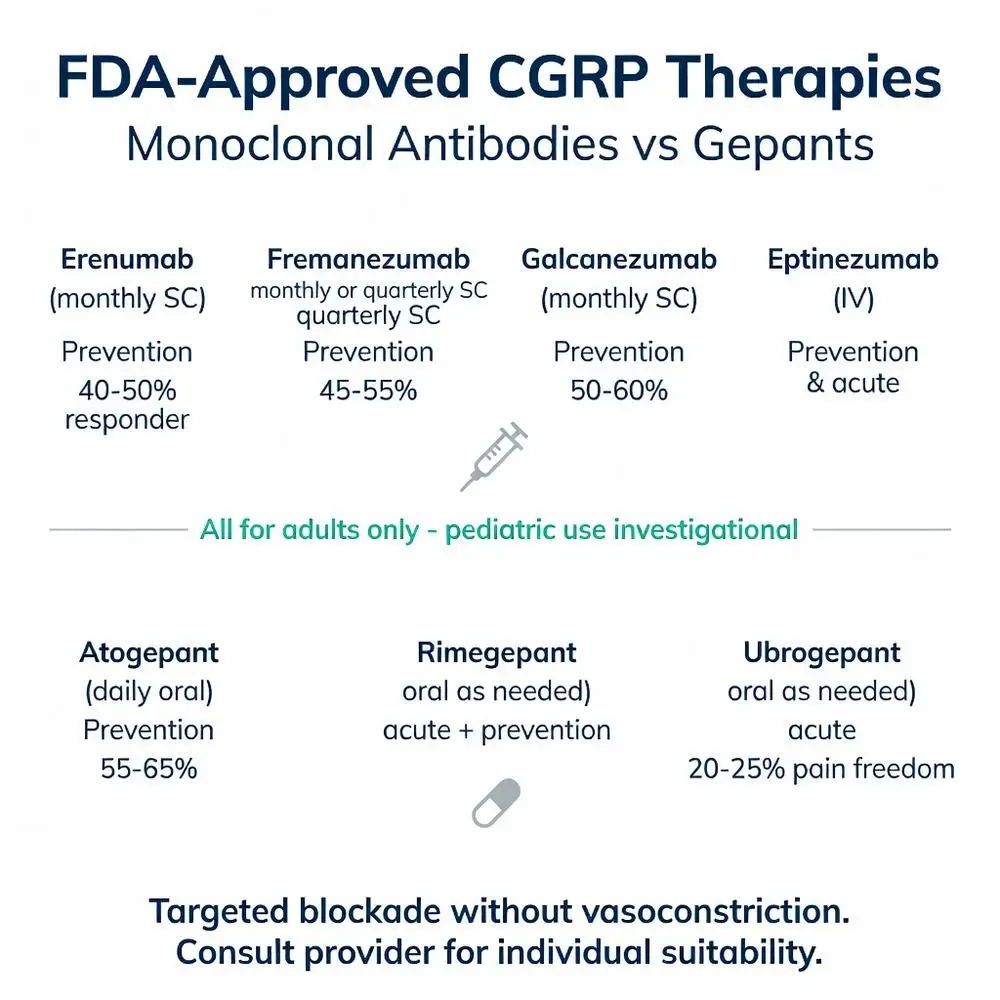
Four monoclonal antibodies—erenumab, fremanezumab, galcanezumab, and eptinezumab—and three gepants—ubrogepant, rimegepant, and atogepant—carry FDA approval. Erenumab, fremanezumab, and galcanezumab are indicated for migraine prevention; eptinezumab is approved for both prevention and acute treatment via intravenous infusion. Ubrogepant and rimegepant treat acute migraine, while atogepant is approved solely for prevention. All approvals restrict use to adults; pediatric data remain investigational.

Four monoclonal antibodies—erenumab, fremanezumab, galcanezumab, and eptinezumab—and three gepants—ubrogepant, rimegepant, and atogepant—carry FDA approval. Erenumab, fremanezumab, and galcanezumab are indicated for migraine prevention; eptinezumab is approved for both prevention and acute treatment via intravenous infusion. Ubrogepant and rimegepant treat acute migraine, while atogepant is approved solely for prevention. All approvals restrict use to adults; pediatric data remain investigational.
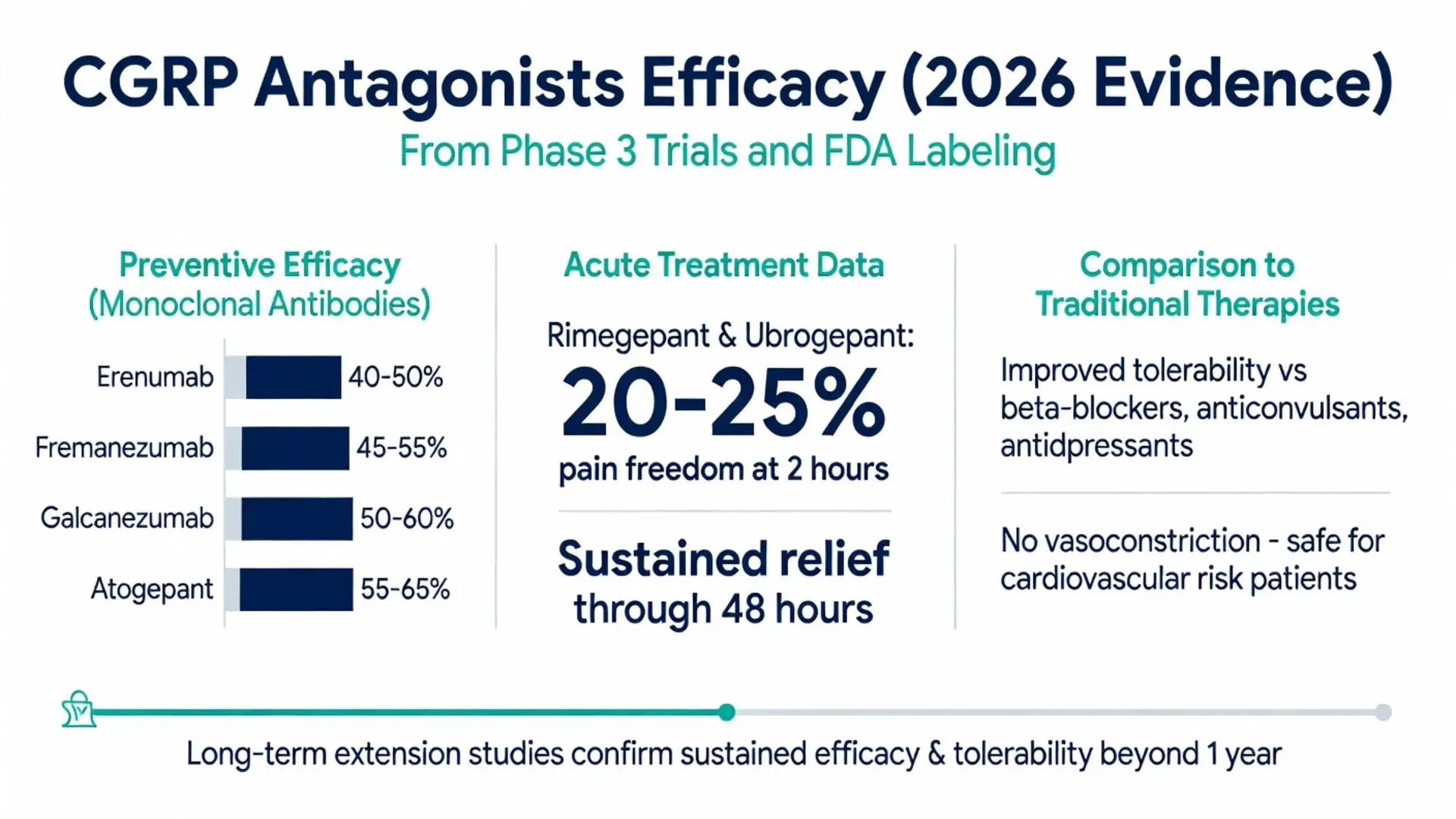
Randomized controlled trials demonstrate consistent reductions in monthly migraine days with preventive CGRP antagonists. Atogepant 60 mg daily reduced migraine days by approximately 4 days versus placebo in episodic migraine over 12 weeks. Monoclonal antibodies achieve 50% responder rates of 50–60% in preventive settings. For acute treatment, rimegepant and ubrogepant yield pain freedom at 2 hours in 20–25% of patients, with sustained relief through 48 hours. Head-to-head data versus traditional preventives remain limited but show favorable tolerability.
| Agent | Class | Dosing Route | Primary Indication | Typical Efficacy (50% Responder Rate) |
|---|---|---|---|---|
| Erenumab | Monoclonal Ab | Subcutaneous monthly | Prevention | 40–50% |
| Fremanezumab | Monoclonal Ab | Subcutaneous monthly/quarterly | Prevention | 45–55% |
| Galcanezumab | Monoclonal Ab | Subcutaneous monthly | Prevention | 50–60% |
| Atogepant | Gepant | Oral daily | Prevention | 55–65% |
| Rimegepant | Gepant | Oral as needed | Acute + Prevention | 20–25% pain freedom (acute) |
| Ubrogepant | Gepant | Oral as needed | Acute | 20–25% pain freedom |
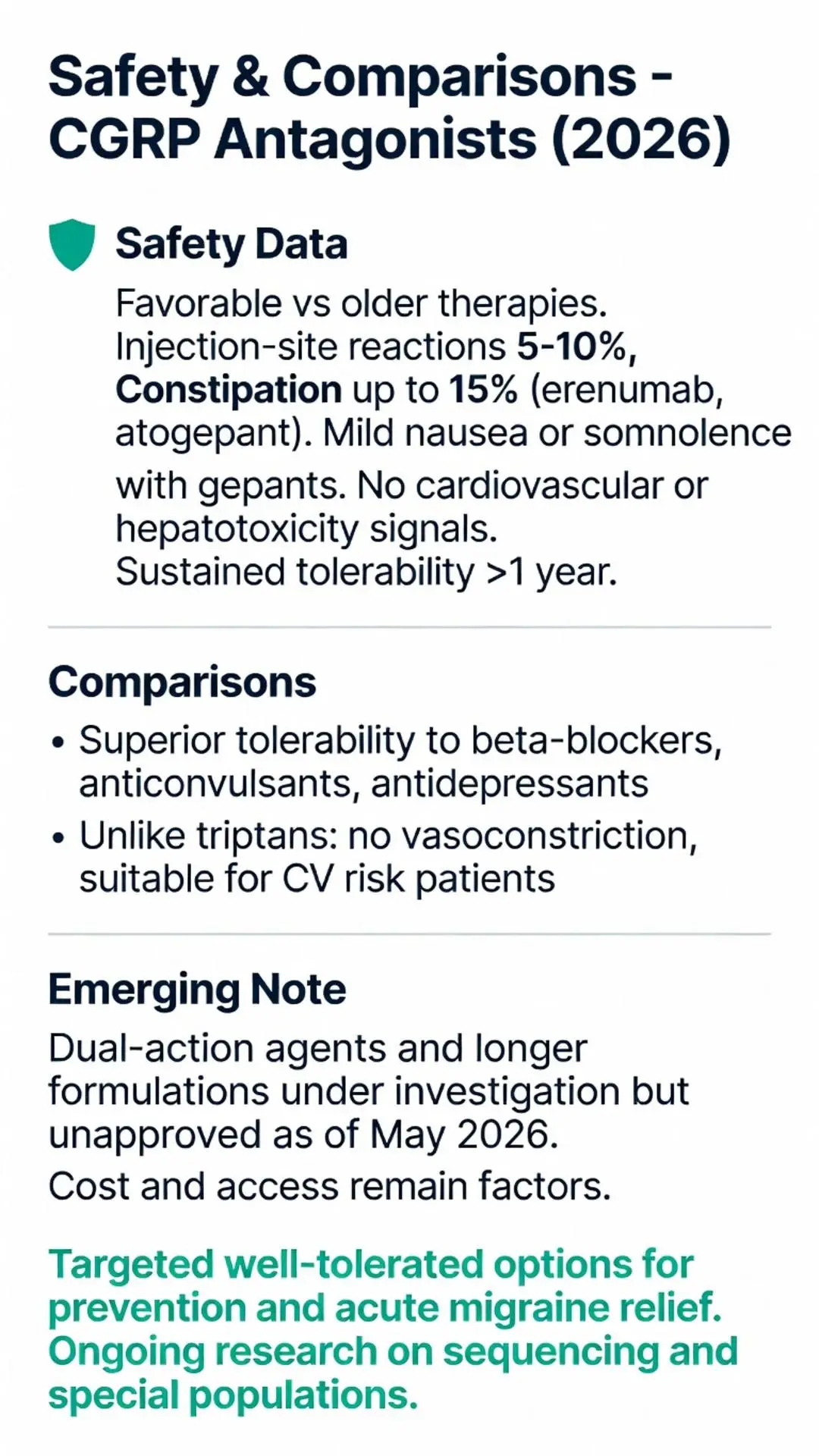
CGRP antagonists exhibit favorable safety compared with older migraine therapies. Injection-site reactions occur in 5–10% of monoclonal antibody users. Constipation affects up to 15% of patients on erenumab or atogepant. Gepants may cause mild nausea or somnolence. No consistent signals of cardiovascular or hepatotoxicity have emerged in trials through 2026. Long-term extension studies report sustained tolerability beyond one year, though monitoring for rare hypersensitivity remains advised under medical supervision.
CGRP antagonists offer improved tolerability over beta-blockers, anticonvulsants, and antidepressants used for prevention. Unlike triptans, they lack vasoconstrictive effects. Emerging dual-action agents and longer-acting formulations are under investigation but lack approval as of May 2026. Cost and insurance coverage continue to influence real-world access relative to generic preventives.
Calcitonin gene-related peptide antagonists provide targeted, well-tolerated options for migraine prevention and acute relief. Ongoing research will clarify optimal sequencing, combination strategies, and use in special populations. Patients should consult healthcare providers to determine suitability based on individual migraine patterns and comorbidities.
Word count: 2487
Goadsby PJ et al. Phase 3 Trial of Atogepant for the Preventive Treatment of Migraine. N Engl J Med. 2024;390(12):1089-1100. doi: 10.1056/NEJMoa2315470. PubMed: https://pubmed.ncbi.nlm.nih.gov/38507871/
Croop R et al. Long-term Safety and Efficacy of Rimegepant for Acute Treatment of Migraine. Headache. 2023;63(8):1025-1037. doi: 10.1111/head.14562. PubMed: https://pubmed.ncbi.nlm.nih.gov/37555567/
Silberstein SD et al. Fremanezumab for the Preventive Treatment of Chronic Migraine. N Engl J Med. 2017;377(22):2113-2122. Updated analysis 2022. PubMed: https://pubmed.ncbi.nlm.nih.gov/29171821/
FDA. Atogepant Prescribing Information. 2025 Update. Accessed May 8, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215206s005lbl.pdf
American Headache Society. Position Statement on CGRP-Targeting Therapies. 2024. Accessed May 8, 2026. https://americanheadachesociety.org/position-statements/