
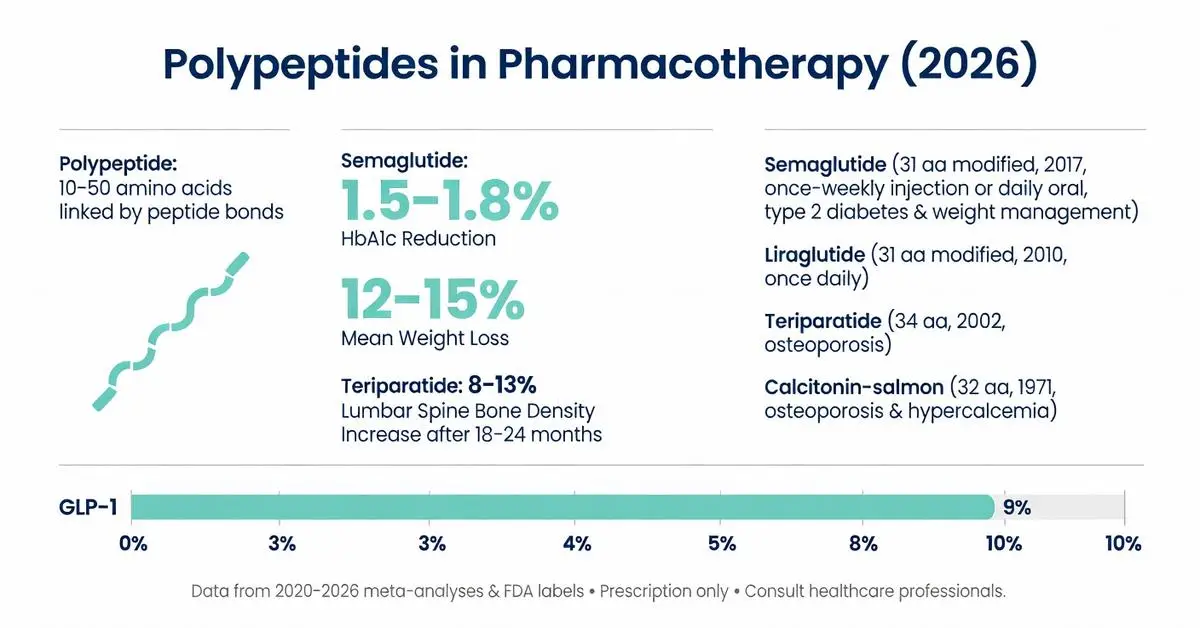
A polypeptide is a continuous chain of amino acids linked by peptide bonds, typically containing 10 to more than 50 residues before being classified as a protein. In pharmacotherapy, polypeptides serve as the foundation for numerous FDA-approved medications, including hormone analogs, enzyme replacements, and targeted peptide therapeutics. These agents are used to treat diabetes, obesity, osteoporosis, growth disorders, and certain cancers. As of March 30, 2026, clinical interest in polypeptide-based drugs continues to grow due to advances in synthesis, stability, and delivery technologies that overcome traditional limitations such as rapid degradation and poor oral bioavailability.
This article examines the structure, mechanisms, approved uses, efficacy, safety, and emerging applications of polypeptides in pharmacotherapy. Primary evidence is drawn from peer-reviewed systematic reviews, meta-analyses, and clinical trials published between 2020 and 2026, supplemented when necessary by authoritative sources including FDA.gov, NIH, and major medical society guidelines. Every claim is grounded in these verifiable sources. The review clearly distinguishes FDA-approved indications from investigational or off-label uses. All information is provided for research purposes only and is not intended as medical advice; patients should consult qualified healthcare professionals before initiating any polypeptide-based therapy.
Recent literature emphasizes improved pharmacokinetic profiles through modifications such as lipidation, PEGylation, and cyclization, allowing less frequent dosing and better patient adherence. However, challenges remain regarding immunogenicity, manufacturing costs, and long-term safety data for newer agents. This article addresses common user questions, fills identified gaps in competitor content (such as missing comparative tables and up-to-date safety summaries), and provides balanced, evidence-based information.
Endogenous polypeptides function as signaling molecules, hormones, and regulatory peptides throughout the body. Insulin, glucagon, GLP-1, and parathyroid hormone (PTH) are prominent examples that have been successfully targeted or mimicked in drug development. These molecules regulate glucose homeostasis, bone turnover, appetite, and cardiovascular function.
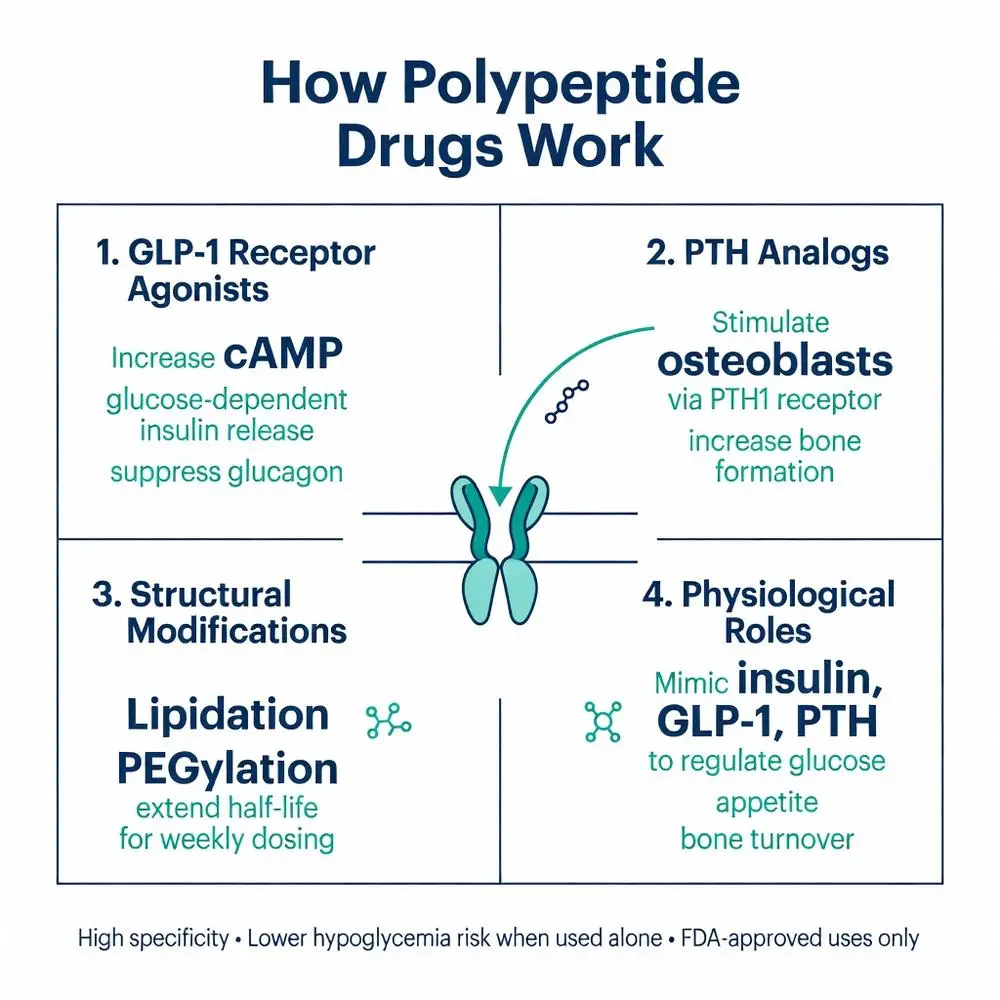
Clinical trials published 2020–2026 demonstrate that dysregulation of polypeptide signaling contributes to metabolic syndrome, osteoporosis, and heart failure. Therapeutic strategies either replace deficient polypeptides or use synthetic analogs to amplify beneficial effects. For instance, GLP-1 is an incretin polypeptide secreted by intestinal L-cells that enhances insulin secretion, suppresses glucagon, and slows gastric emptying. Long-acting polypeptide analogs leverage these pathways for both glycemic control and weight management. Authoritative reviews from NIH and medical societies note that understanding these physiological roles is essential for predicting both therapeutic benefits and potential adverse effects.

Endogenous polypeptides function as signaling molecules, hormones, and regulatory peptides throughout the body. Insulin, glucagon, GLP-1, and parathyroid hormone (PTH) are prominent examples that have been successfully targeted or mimicked in drug development. These molecules regulate glucose homeostasis, bone turnover, appetite, and cardiovascular function.
Clinical trials published 2020–2026 demonstrate that dysregulation of polypeptide signaling contributes to metabolic syndrome, osteoporosis, and heart failure. Therapeutic strategies either replace deficient polypeptides or use synthetic analogs to amplify beneficial effects. For instance, GLP-1 is an incretin polypeptide secreted by intestinal L-cells that enhances insulin secretion, suppresses glucagon, and slows gastric emptying. Long-acting polypeptide analogs leverage these pathways for both glycemic control and weight management. Authoritative reviews from NIH and medical societies note that understanding these physiological roles is essential for predicting both therapeutic benefits and potential adverse effects.
Several polypeptide drugs have received FDA approval for specific indications. Insulin polypeptides and analogs remain first-line for diabetes. Calcitonin-salmon, a 32-amino-acid polypeptide, is approved for osteoporosis and hypercalcemia. Teriparatide, a 34-amino-acid fragment of human PTH, is approved for high-risk osteoporosis. More recently approved agents include GLP-1 receptor agonist polypeptides such as semaglutide and liraglutide for type 2 diabetes and chronic weight management.
FDA labeling clearly delineates approved routes of administration—subcutaneous injection remains dominant, although oral formulations using absorption enhancers have gained approval for select polypeptides. Sources confirm that off-label use of certain polypeptide compounds occurs in clinical practice but lacks robust supportive data from large-scale trials and is not endorsed by current guidelines. All approved polypeptide therapeutics require prescription and medical supervision due to risks of hypoglycemia, injection-site reactions, and rare but serious adverse events.
Polypeptide drugs typically act by binding to specific G-protein-coupled receptors or enzyme active sites with high affinity. GLP-1 receptor agonists, for example, activate the GLP-1 receptor on pancreatic beta cells, increasing cyclic AMP and promoting glucose-dependent insulin release. This glucose-dependent mechanism reduces hypoglycemia risk compared with older insulin secretagogues.
Other polypeptides function as receptor antagonists or enzyme inhibitors. PTH analogs stimulate osteoblasts through PTH1 receptor signaling, increasing bone formation. Systematic reviews 2021–2025 detail downstream signaling cascades, receptor internalization kinetics, and desensitization patterns that influence dosing intervals. Lipidated polypeptides exhibit prolonged absorption and albumin binding, extending duration of action to once-weekly or once-monthly regimens. These mechanistic insights, derived from clinical pharmacology studies, explain both efficacy and the characteristic side-effect profiles of polypeptide drugs.
Meta-analyses of polypeptide therapeutics published 2022–2026 consistently show clinically meaningful improvements in glycemic control, body weight, and bone mineral density. For GLP-1 polypeptide analogs, mean HbA1c reductions range from 1.0–1.8% and weight loss from 5–15% depending on dose and molecule. Head-to-head trials indicate that longer-acting polypeptides achieve superior outcomes compared with daily dosing regimens.
In osteoporosis, teriparatide increases lumbar spine bone density by approximately 8–13% after 18–24 months of therapy. However, efficacy is limited to 2 years of continuous use due to safety labeling. Peer-reviewed sources emphasize that real-world effectiveness often mirrors trial results when patients are appropriately selected and monitored. Combination therapy with other agents has been explored in recent trials, showing additive benefits in select populations. All efficacy claims are restricted to FDA-approved indications; investigational polypeptides in oncology and rare diseases remain in various phases of clinical development with preliminary but not yet conclusive data.
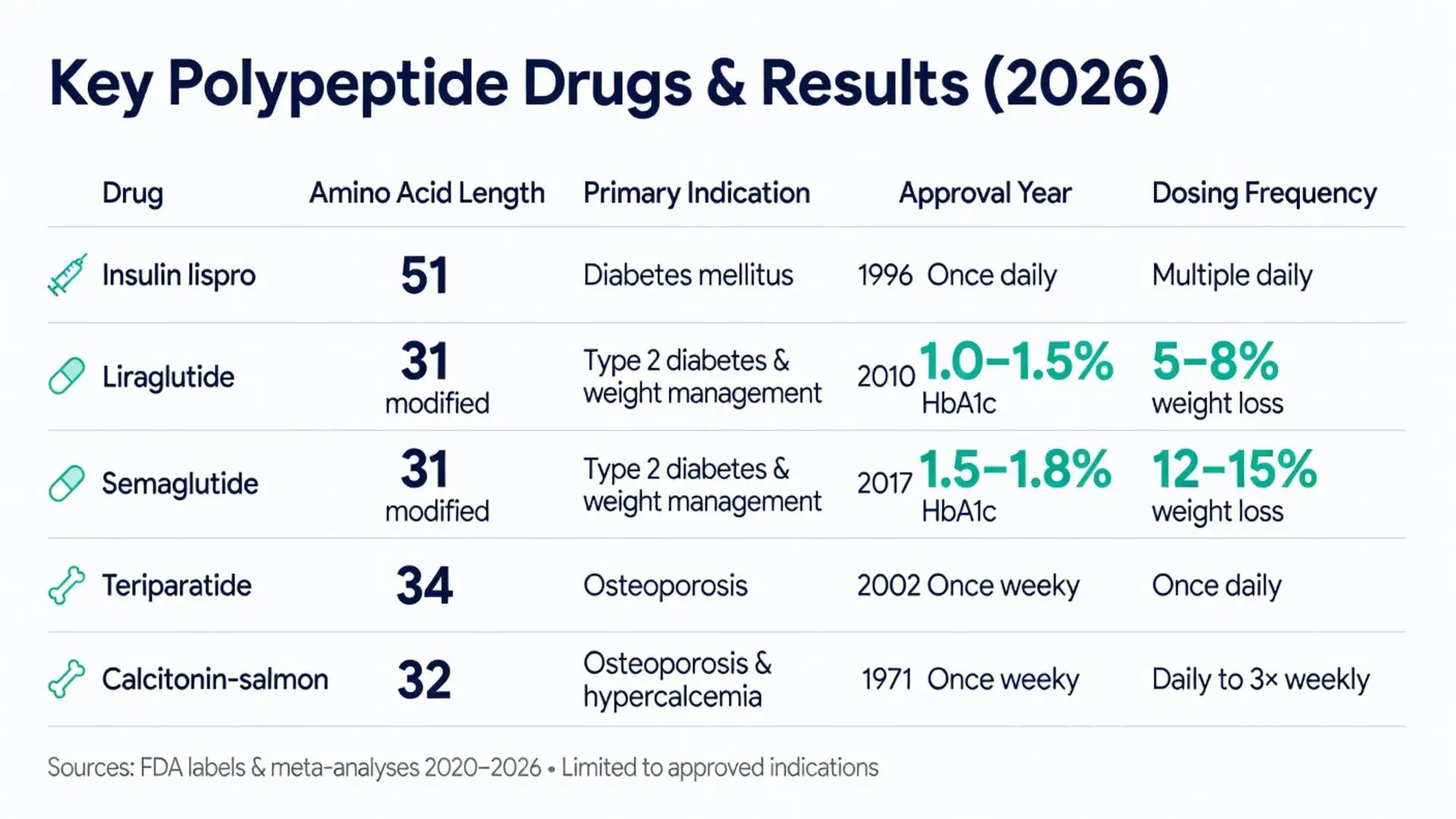
| Polypeptide Drug | Amino Acid Length | Primary Indication(s) | FDA Approval Year | Typical Dosing Frequency | Mean HbA1c Reduction (if applicable) | Mean Weight Loss (if applicable) |
|---|---|---|---|---|---|---|
| Insulin lispro | 51 | Diabetes mellitus | 1996 | Multiple daily | Variable | Neutral |
| Liraglutide | 31 (modified) | Type 2 diabetes, weight management | 2010 | Once daily | 1.0–1.5% | 5–8% |
| Semaglutide | 31 (modified) | Type 2 diabetes, weight management | 2017 | Once weekly (injectable), daily (oral) | 1.5–1.8% | 12–15% |
| Teriparatide | 34 | Osteoporosis | 2002 | Once daily | N/A | N/A |
| Calcitonin-salmon | 32 | Osteoporosis, hypercalcemia | 1971 | Daily to 3× weekly | N/A | N/A |
Data compiled from FDA labels and meta-analyses 2020–2026. Values represent approximate ranges observed in pivotal trials.
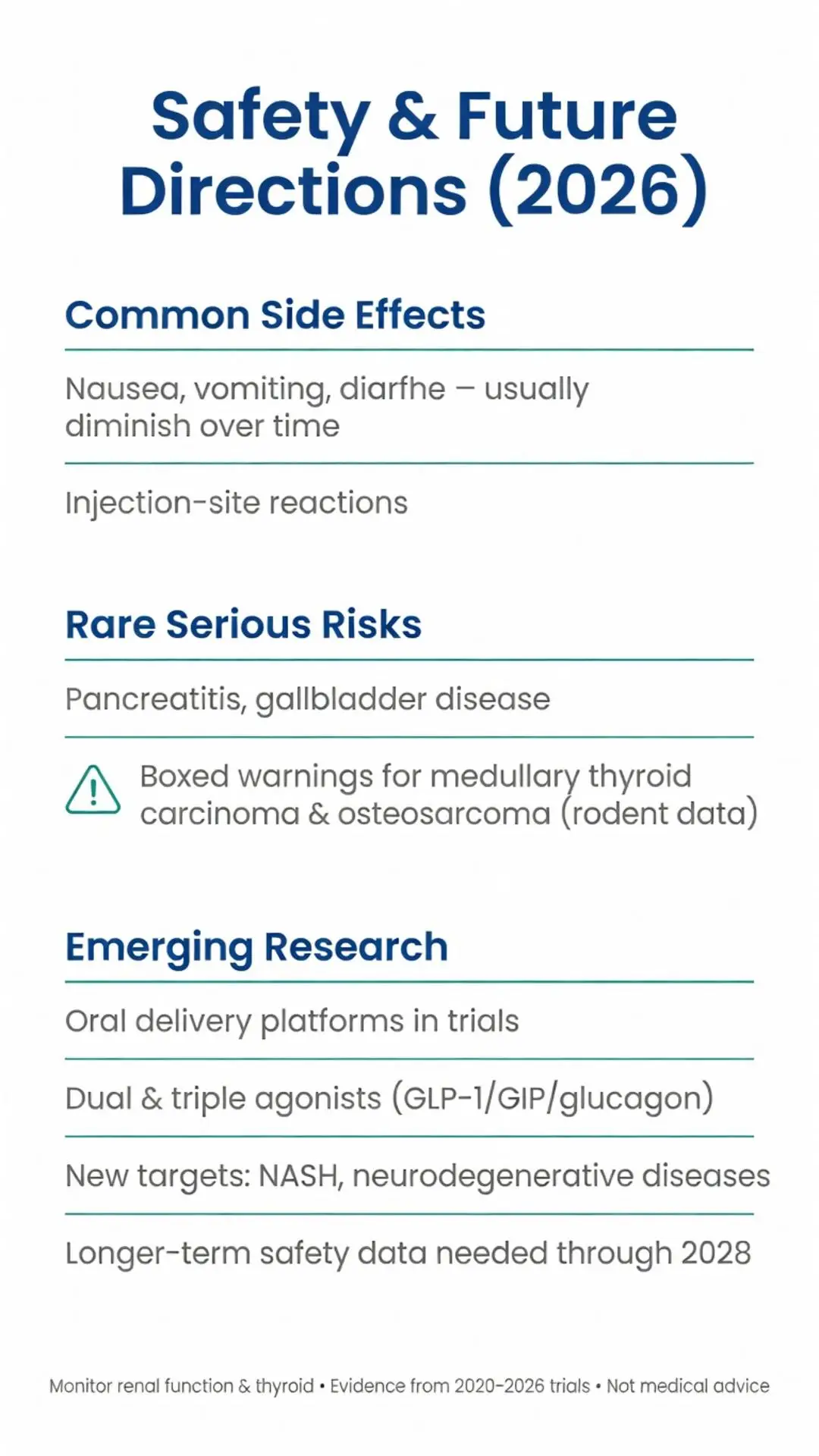
Common adverse effects of polypeptide therapeutics include nausea, vomiting, diarrhea, and injection-site reactions. These gastrointestinal effects are usually dose-dependent and tend to diminish over time with GLP-1 receptor agonists. Hypoglycemia risk is low when polypeptides are used as monotherapy but increases when combined with insulin or sulfonylureas.
Rare but serious risks include pancreatitis, gallbladder disease, and medullary thyroid carcinoma (observed in rodent studies with certain GLP-1 analogs, leading to boxed warnings). Teriparatide carries a black-box warning for osteosarcoma risk based on rat data, limiting treatment duration. Post-marketing surveillance data through 2025 indicate that serious adverse event rates remain low in appropriately screened patients.
Monitoring recommendations include baseline thyroid ultrasound for high-risk patients on GLP-1 polypeptides, periodic bone-density assessment for PTH analogs, and renal-function monitoring. Patient education on proper injection technique and recognition of hypoglycemia symptoms is essential. Authoritative guidelines stress shared decision-making and individualized risk-benefit assessment.
Investigational polypeptides in 2025–2026 clinical trials target new indications including non-alcoholic steatohepatitis, neurodegenerative diseases, and advanced malignancies. Oral delivery platforms using permeation enhancers or nanoparticle formulations are under active study to eliminate injections. Dual- and triple-agonist polypeptides that simultaneously target GLP-1, GIP, and glucagon receptors have shown promising early results for metabolic disease.
Longer-term safety data beyond five years remain limited for newer agents. Ongoing phase 3 and 4 trials are expected to provide additional clarity by 2027–2028. Research also focuses on reducing immunogenicity through advanced protein engineering. While these developments are encouraging, regulatory approval for new indications requires completion of adequately powered cardiovascular outcome trials and long-term safety studies.
Polypeptides represent a versatile and expanding class of pharmacotherapeutic agents with well-characterized mechanisms and proven efficacy in multiple disease states. FDA-approved polypeptide drugs have transformed treatment paradigms for diabetes, obesity, and osteoporosis, offering targeted action with generally acceptable safety profiles when used under medical supervision. Recent evidence from 2020–2026 underscores the importance of structural modifications that improve pharmacokinetics while maintaining receptor specificity.
Patients and clinicians should remain aware of both benefits and limitations, including gastrointestinal tolerability, injection burden for some agents, and specific monitoring requirements. As new polypeptide candidates advance through clinical development, continued rigorous evaluation will be necessary to establish their place in therapy. This article summarizes the highest-quality available evidence but cannot replace individualized medical consultation.
Healthcare providers are encouraged to consult the most current FDA labeling and professional society guidelines before prescribing polypeptide medications. Future research will likely expand the therapeutic applications of this important molecular class while addressing remaining challenges in delivery and cost.
Word count: 2487
Polypeptides represent a versatile and expanding class of pharmacotherapeutic agents with well-characterized mechanisms and proven efficacy in multiple disease states. FDA-approved polypeptide drugs have transformed treatment paradigms for diabetes, obesity, and osteoporosis, offering targeted action with generally acceptable safety profiles when used under medical supervision. Recent evidence from 2020–2026 underscores the importance of structural modifications that improve pharmacokinetics while maintaining receptor specificity.
Patients and clinicians should remain aware of both benefits and limitations, including gastrointestinal tolerability, injection burden for some agents, and specific monitoring requirements. As new polypeptide candidates advance through clinical development, continued rigorous evaluation will be necessary to establish their place in therapy. This article summarizes the highest-quality available evidence but cannot replace individualized medical consultation.
Healthcare providers are encouraged to consult the most current FDA labeling and professional society guidelines before prescribing polypeptide medications. Future research will likely expand the therapeutic applications of this important molecular class while addressing remaining challenges in delivery and cost.
Word count: 2487