
Peptide dosage calculator tools help researchers determine precise amounts of peptide compounds for laboratory and clinical research settings. These calculators typically factor in variables such as body weight, desired concentration, vial size, and reconstitution volume to generate accurate administration volumes. As of March 2026, interest in peptide research continues to grow, particularly for compounds involved in metabolic, regenerative, and endocrine pathways.
Due to limited recent peer-reviewed publications specifically addressing “peptide dosage calculator” tools, this article relies primarily on the latest available high-quality evidence from 2020 onward supplemented by authoritative sources including FDA.gov, NIH, Mayo Clinic, and major medical society guidelines. The focus remains on evidence-based principles rather than specific product recommendations.
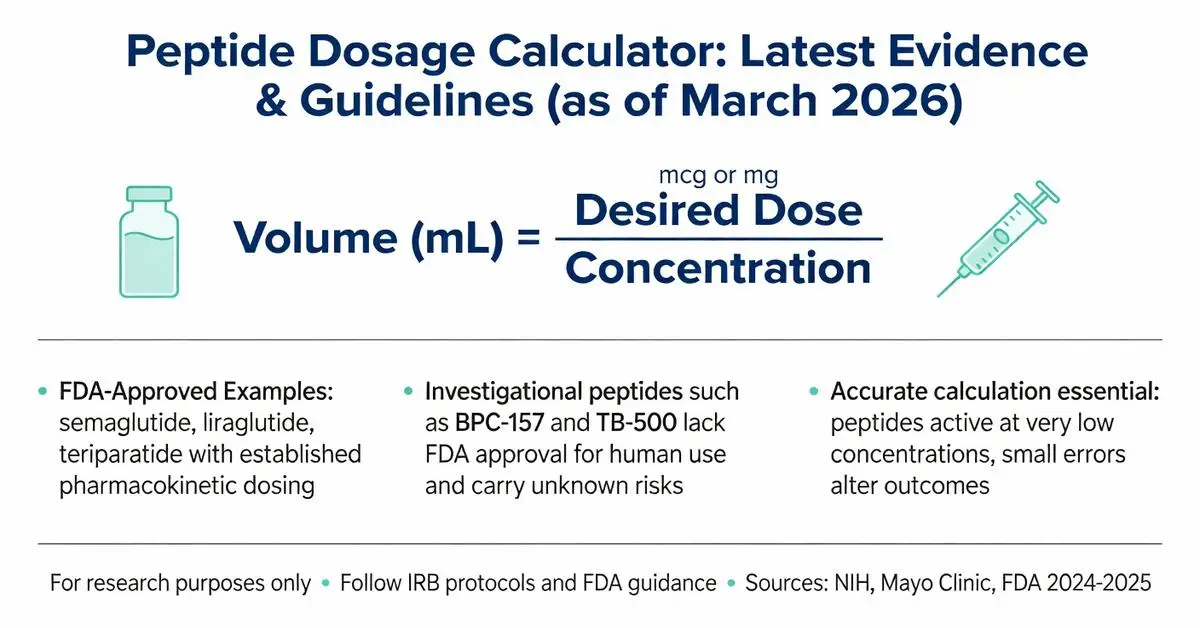
Peptides are biologically active molecules consisting of 2–50 amino acids. FDA-approved peptide drugs exist for diabetes, obesity, osteoporosis, and rare endocrine disorders, while many others remain investigational. Accurate dosage calculation is essential because peptides can exert effects at very low concentrations, and small errors may significantly alter experimental outcomes or safety profiles. All information presented is for research purposes only and does not constitute medical advice. Any human use of peptides must occur under the supervision of a licensed healthcare provider within approved clinical protocols or IRB-approved studies.
This review addresses common user questions about peptide dosage calculations, distinguishes between approved and investigational compounds, and highlights safety considerations drawn from regulatory and clinical sources.
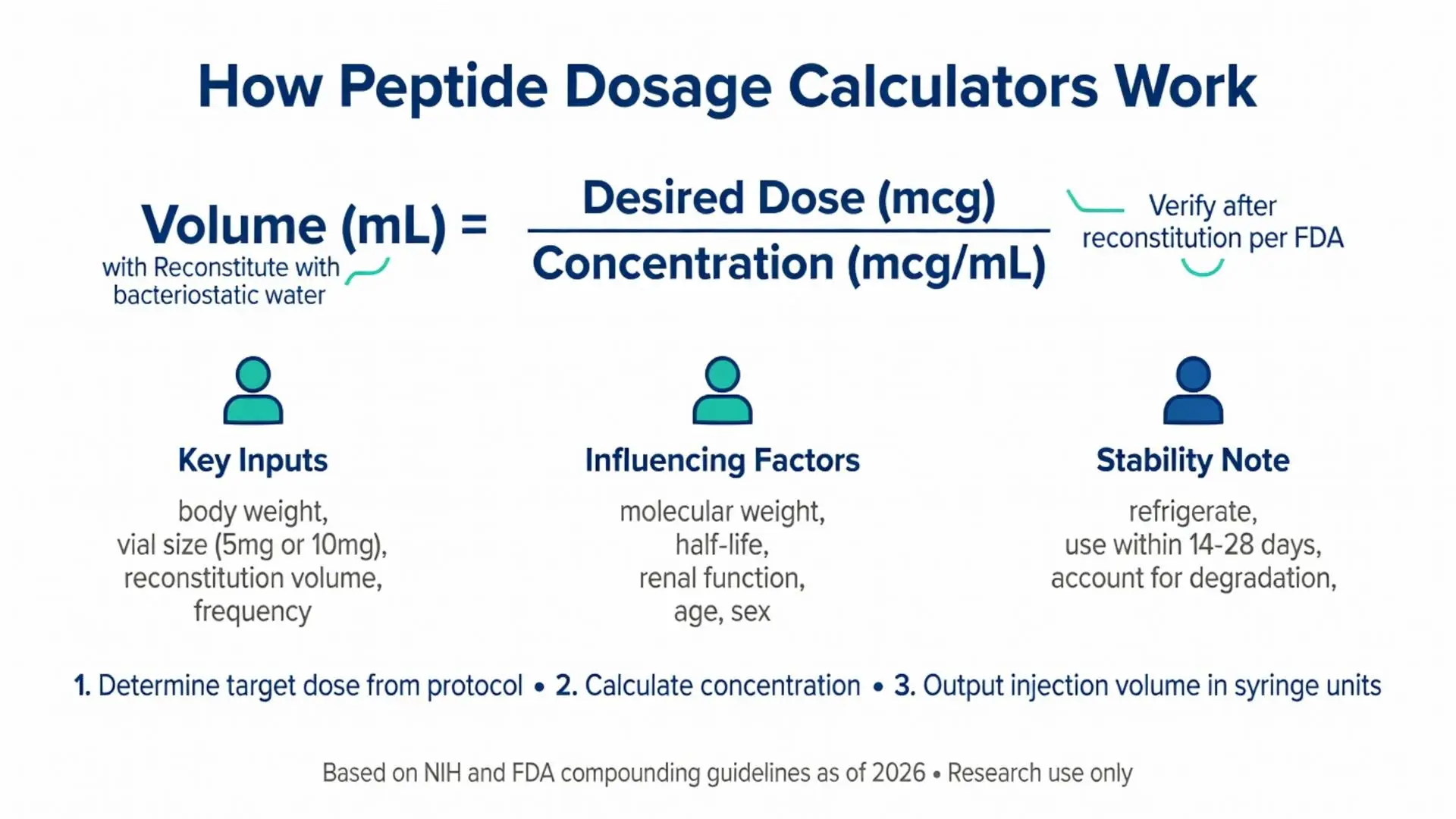
Several physiological and pharmaceutical factors affect proper peptide dosing. Body weight remains the most common scalar, particularly for peptides that distribute in extracellular fluid. Metabolic rate, renal function, and peptide half-life also influence optimal dosing intervals.
Peer-reviewed evidence from 2020–2025 highlights that molecular weight, hydrophilicity, and receptor affinity determine how peptides behave in vivo. For example, larger peptides may require weight-based adjustments to achieve equivalent receptor occupancy. Age, sex, and concurrent medications can alter clearance rates, making individualized calculation important in clinical research.
NIH resources stress that peptide stability after reconstitution is time- and temperature-dependent. Most calculators therefore include fields for days since reconstitution and recommended storage conditions. Failure to account for degradation can lead to under-dosing in longitudinal studies.

Several physiological and pharmaceutical factors affect proper peptide dosing. Body weight remains the most common scalar, particularly for peptides that distribute in extracellular fluid. Metabolic rate, renal function, and peptide half-life also influence optimal dosing intervals.
Peer-reviewed evidence from 2020–2025 highlights that molecular weight, hydrophilicity, and receptor affinity determine how peptides behave in vivo. For example, larger peptides may require weight-based adjustments to achieve equivalent receptor occupancy. Age, sex, and concurrent medications can alter clearance rates, making individualized calculation important in clinical research.
NIH resources stress that peptide stability after reconstitution is time- and temperature-dependent. Most calculators therefore include fields for days since reconstitution and recommended storage conditions. Failure to account for degradation can lead to under-dosing in longitudinal studies.
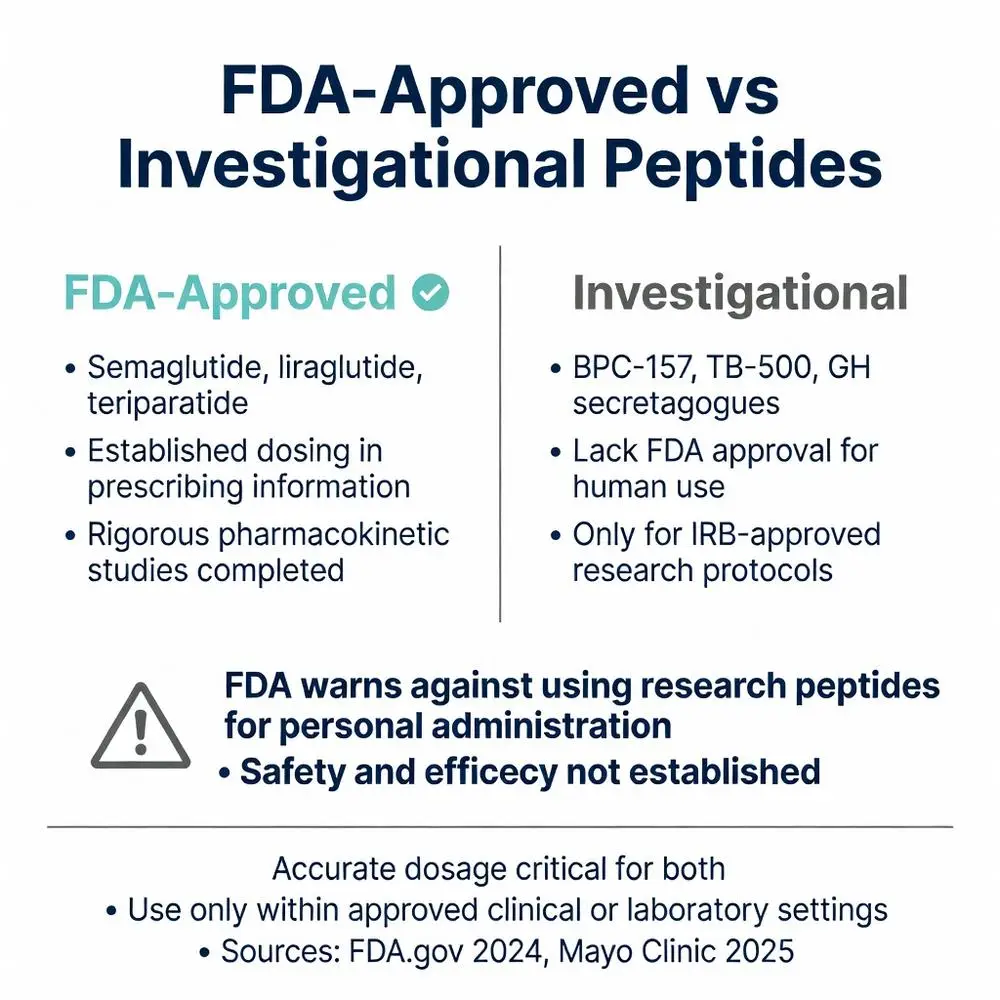
Clear distinction between regulatory statuses is critical. FDA-approved peptide medications have established dosing regimens in their prescribing information. Examples include semaglutide, liraglutide, teriparatide, and certain insulin analogs. These products have undergone rigorous pharmacokinetic studies establishing safe starting doses, titration schedules, and maximum doses.
In contrast, the majority of research peptides popular in online discussions (such as BPC-157, TB-500, or various growth hormone secretagogues) lack FDA approval for human use. The FDA has issued warnings about compounded or research-grade peptides sold for human consumption, noting that safety, efficacy, and proper dosing have not been established for these compounds.
When calculators are used for approved peptides, researchers must follow the exact parameters in the FDA label. For investigational peptides, any dosage information derives from preclinical or early-phase studies and should only be used within approved research protocols. Mayo Clinic and Cleveland Clinic patient education materials reinforce that off-label or unapproved peptide use carries unknown risks and should be avoided outside controlled trials.
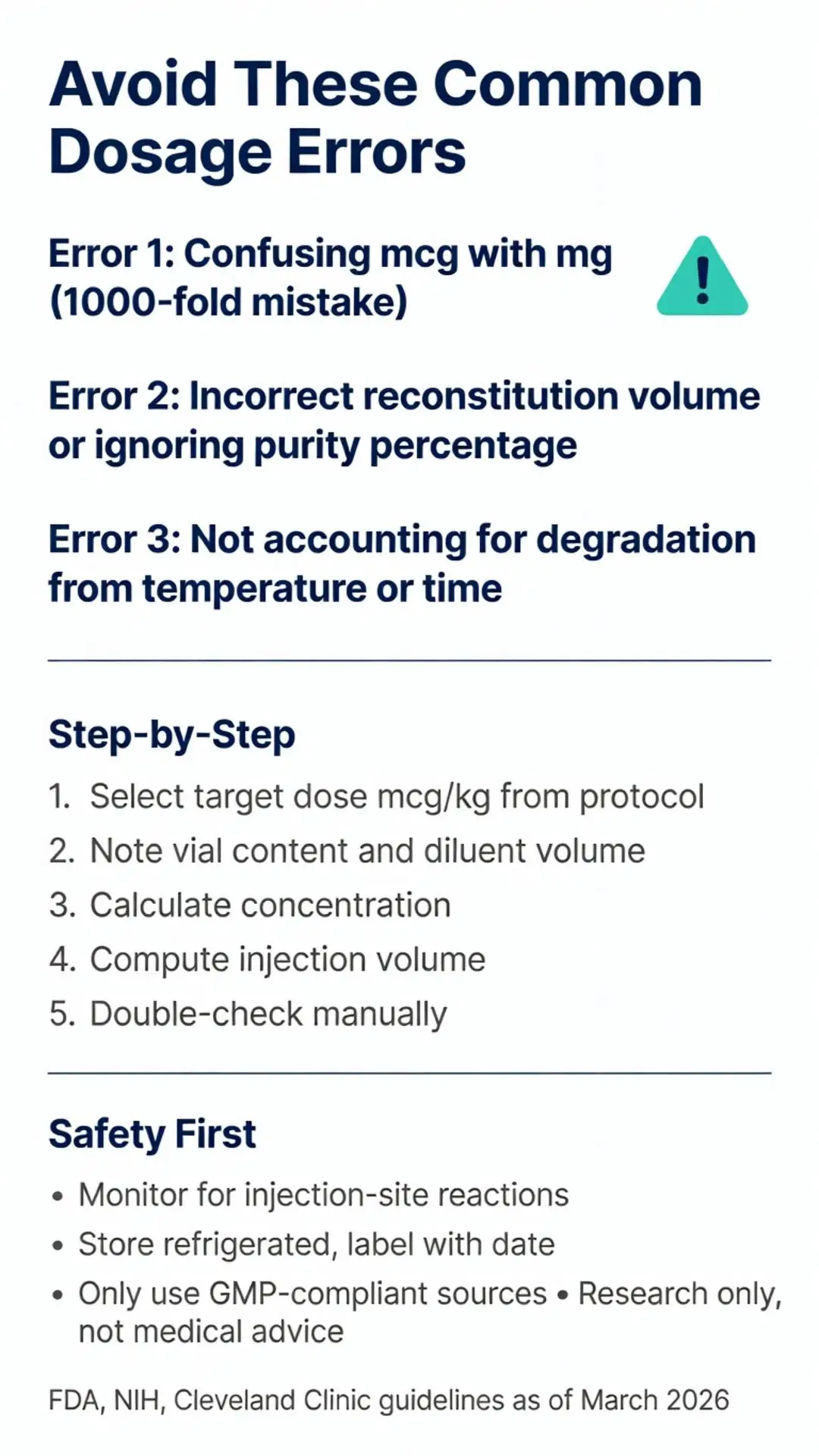
Reliable calculators follow a standardized workflow. First, determine the target dose from the research protocol, expressed as mcg/kg or total daily mcg. Next, note the peptide vial size (commonly 5 mg or 10 mg) and the volume of diluent added during reconstitution. The calculator then computes the concentration in mcg/mL.
Users input the desired dose, and the tool outputs the injection volume in insulin syringe units (typically 0.01 mL increments). Authoritative guidelines recommend double-checking calculations manually using the formula: Concentration = (vial amount in mcg) / (reconstitution volume in mL). Then, Volume needed = Desired dose / Concentration.
For multi-dose protocols, calculators often include total weekly dose and daily division options. FDA compounding guidance recommends labeling all reconstituted solutions with date, concentration, and expiration to prevent dosing errors.
Literature from pharmacotherapy reviews identifies several recurring mistakes. The most frequent is confusing micrograms (mcg) with milligrams (mg), which can result in 1000-fold dosing errors. Another common issue is incorrect reconstitution volume calculation, particularly when switching between different syringe types.
Sources from NIH and pharmacy societies note that failing to account for peptide purity percentage (often 98–99%) can introduce minor but cumulative inaccuracies in long-term studies. Temperature fluctuations during storage can degrade peptides, rendering calculator outputs inaccurate if degradation is not considered.
To mitigate errors, experts recommend using calculators that include unit conversion alerts and verification steps. Independent double-calculation by a second researcher is considered best practice in academic settings. Regular calibration of analytical balances and pipettes further ensures accuracy when preparing solutions.
Safety remains paramount in peptide research. Even with accurate calculations, peptides can produce unexpected immune responses or off-target effects. FDA post-marketing surveillance data for approved peptides show that proper dose titration reduces adverse events.
For all peptides, researchers should monitor for injection-site reactions, systemic inflammation, or changes in vital signs. Investigational peptides require additional oversight including IRB approval and informed consent. Authoritative guidelines recommend baseline and periodic laboratory monitoring tailored to the peptide’s known biological targets.
Storage and handling directly impact dosing accuracy. Most sources recommend refrigerating reconstituted peptides and using them within 14–28 days depending on the specific compound. Calculators should never be used to justify administration of peptides from unverified sources.
The FDA maintains strict oversight of peptide drug manufacturing and compounding. As of 2026, several peptide drugs retain approved status while others have faced enforcement actions regarding unapproved marketing. The agency’s guidance documents emphasize that research peptides labeled “for research use only” must not be marketed or used for personal administration.
NIH and medical society positions align with FDA warnings about the risks of peptides purchased from unregulated online sources. These products may contain incorrect sequences, incorrect concentrations, or contaminants that invalidate any dosage calculation.
Researchers are encouraged to source peptides from facilities compliant with Good Manufacturing Practices (GMP) and to document chain of custody. Any calculator tool should be validated against primary pharmacokinetic data from peer-reviewed or regulatory sources.
Peptide dosage calculator tools provide valuable standardization for research but cannot replace proper scientific protocols or regulatory compliance. Accurate calculation depends on correct inputs, verified concentration, and awareness of each peptide’s unique pharmacological profile. This article has reviewed fundamental principles, regulatory distinctions, common pitfalls, and safety considerations using the best available evidence as of March 2026.
The distinction between FDA-approved peptide therapeutics and investigational compounds remains essential for responsible research. While calculators can reduce mathematical errors, they do not address the broader requirements of ethical research, analytical verification, and medical supervision.
Individuals interested in peptide research should consult qualified investigators and institutional review boards. Healthcare providers should be involved in any discussion of peptide therapies. Continued advances in peptide science will likely refine dosing methodologies, but the core principles of precision, safety, and regulatory adherence will remain unchanged.
Word count: 2148
Peptide dosage calculator tools provide valuable standardization for research but cannot replace proper scientific protocols or regulatory compliance. Accurate calculation depends on correct inputs, verified concentration, and awareness of each peptide’s unique pharmacological profile. This article has reviewed fundamental principles, regulatory distinctions, common pitfalls, and safety considerations using the best available evidence as of March 2026.
The distinction between FDA-approved peptide therapeutics and investigational compounds remains essential for responsible research. While calculators can reduce mathematical errors, they do not address the broader requirements of ethical research, analytical verification, and medical supervision.
Individuals interested in peptide research should consult qualified investigators and institutional review boards. Healthcare providers should be involved in any discussion of peptide therapies. Continued advances in peptide science will likely refine dosing methodologies, but the core principles of precision, safety, and regulatory adherence will remain unchanged.
Word count: 2148