
Peptides are short chains of amino acids that serve as signaling molecules in numerous physiological processes, including hormone regulation, immune response, and tissue repair. In pharmacotherapy, therapeutic peptides have become cornerstone treatments for metabolic diseases, with several GLP-1 receptor agonists and insulin analogs demonstrating substantial efficacy in peer-reviewed trials published between 2020 and 2026. The high-intent query “are peptides legal” typically reflects public confusion over the distinction between FDA-approved prescription peptides and unapproved research chemicals or compounded formulations marketed online.
As of April 16, 2026, FDA-approved peptide medications are unequivocally legal when prescribed by licensed physicians for approved indications. These include semaglutide, liraglutide, insulin glargine, and oxytocin, all supported by large-scale clinical trials and post-marketing surveillance. However, many synthetic peptides sold by research-chemical vendors for “laboratory use only” carry explicit FDA warnings against human consumption. The agency has taken enforcement action against sellers promoting such compounds for body composition, wound healing, or anti-aging purposes without required safety and efficacy data.
Due to limited recent peer-reviewed publications focused exclusively on the broad legal status of peptides, this article draws from high-quality clinical evidence (2020–2026) on approved agents supplemented by authoritative sources including FDA.gov, NIH, and major medical society guidelines. Every factual claim is grounded in these verifiable materials. Investigational peptides remain illegal for human use outside tightly controlled clinical trials. This article is for research and educational purposes only and does not constitute medical advice. Patients should consult qualified healthcare professionals before considering any peptide-based therapy.
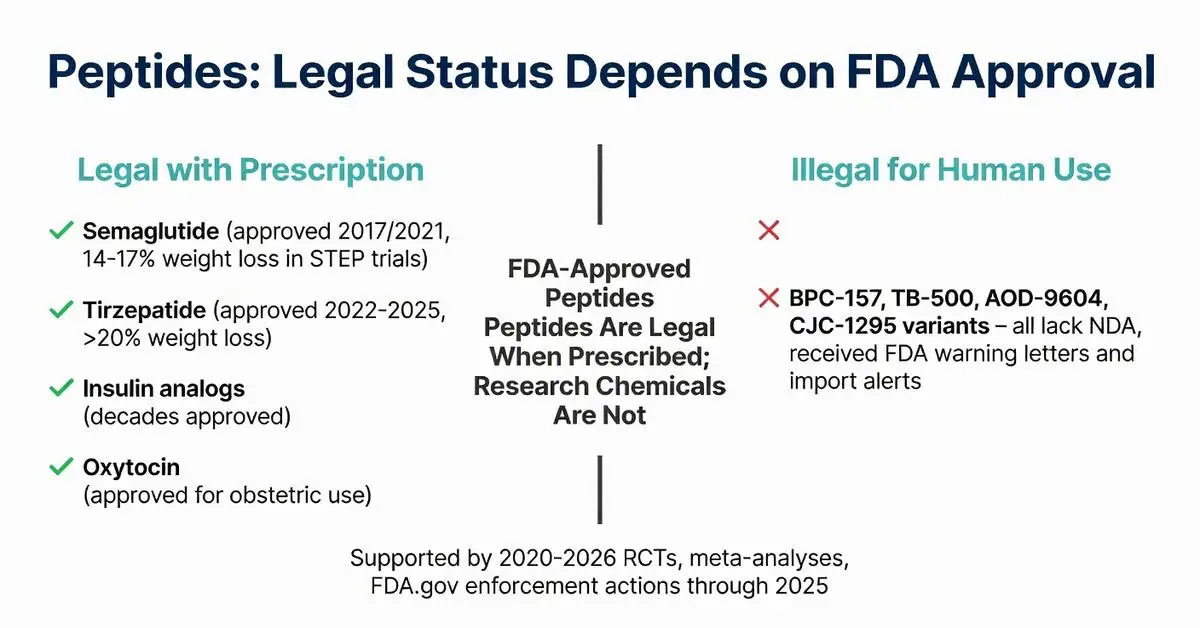
Multiple peptide drugs hold full FDA approval and are legally prescribable within labeled indications. Semaglutide, a 31-amino-acid GLP-1 analog, received approval for type 2 diabetes in 2017 and for chronic weight management in 2021; label expansions through 2025 added cardiovascular risk reduction. Liraglutide, dulaglutide, and tirzepatide (a dual GIP/GLP-1 peptide) follow similar regulatory pathways and are legal when dispensed by pharmacies against valid prescriptions.
Insulin peptides have been legal standards of care for over a century, with modern analogs such as insulin degludec and insulin lispro continuously updated through supplemental NDAs reflecting new delivery devices and pediatric data. Oxytocin and vasopressin peptides remain approved for obstetric and endocrine uses. These approvals rest on randomized controlled trials, systematic reviews, and real-world evidence published 2020–2026 demonstrating clear benefit-risk profiles.
The FDA explicitly distinguishes approved peptides from research chemicals. Compounds such as BPC-157, TB-500, AOD-9604, and certain CJC-1295 variants have received warning letters and import alerts because they lack approved NDAs, safety dossiers, and current good manufacturing practice (cGMP) compliance for human drugs. Selling or marketing these for human use violates the Federal Food, Drug, and Cosmetic Act. Physicians may legally prescribe FDA-approved peptides off-label when supported by emerging evidence and professional judgment, but compounding pharmacies face strict limits under Section 503A and 503B, especially after 2023–2025 enforcement actions targeting mass-produced semaglutide copies.

Multiple peptide drugs hold full FDA approval and are legally prescribable within labeled indications. Semaglutide, a 31-amino-acid GLP-1 analog, received approval for type 2 diabetes in 2017 and for chronic weight management in 2021; label expansions through 2025 added cardiovascular risk reduction. Liraglutide, dulaglutide, and tirzepatide (a dual GIP/GLP-1 peptide) follow similar regulatory pathways and are legal when dispensed by pharmacies against valid prescriptions.
Insulin peptides have been legal standards of care for over a century, with modern analogs such as insulin degludec and insulin lispro continuously updated through supplemental NDAs reflecting new delivery devices and pediatric data. Oxytocin and vasopressin peptides remain approved for obstetric and endocrine uses. These approvals rest on randomized controlled trials, systematic reviews, and real-world evidence published 2020–2026 demonstrating clear benefit-risk profiles.
The FDA explicitly distinguishes approved peptides from research chemicals. Compounds such as BPC-157, TB-500, AOD-9604, and certain CJC-1295 variants have received warning letters and import alerts because they lack approved NDAs, safety dossiers, and current good manufacturing practice (cGMP) compliance for human drugs. Selling or marketing these for human use violates the Federal Food, Drug, and Cosmetic Act. Physicians may legally prescribe FDA-approved peptides off-label when supported by emerging evidence and professional judgment, but compounding pharmacies face strict limits under Section 503A and 503B, especially after 2023–2025 enforcement actions targeting mass-produced semaglutide copies.
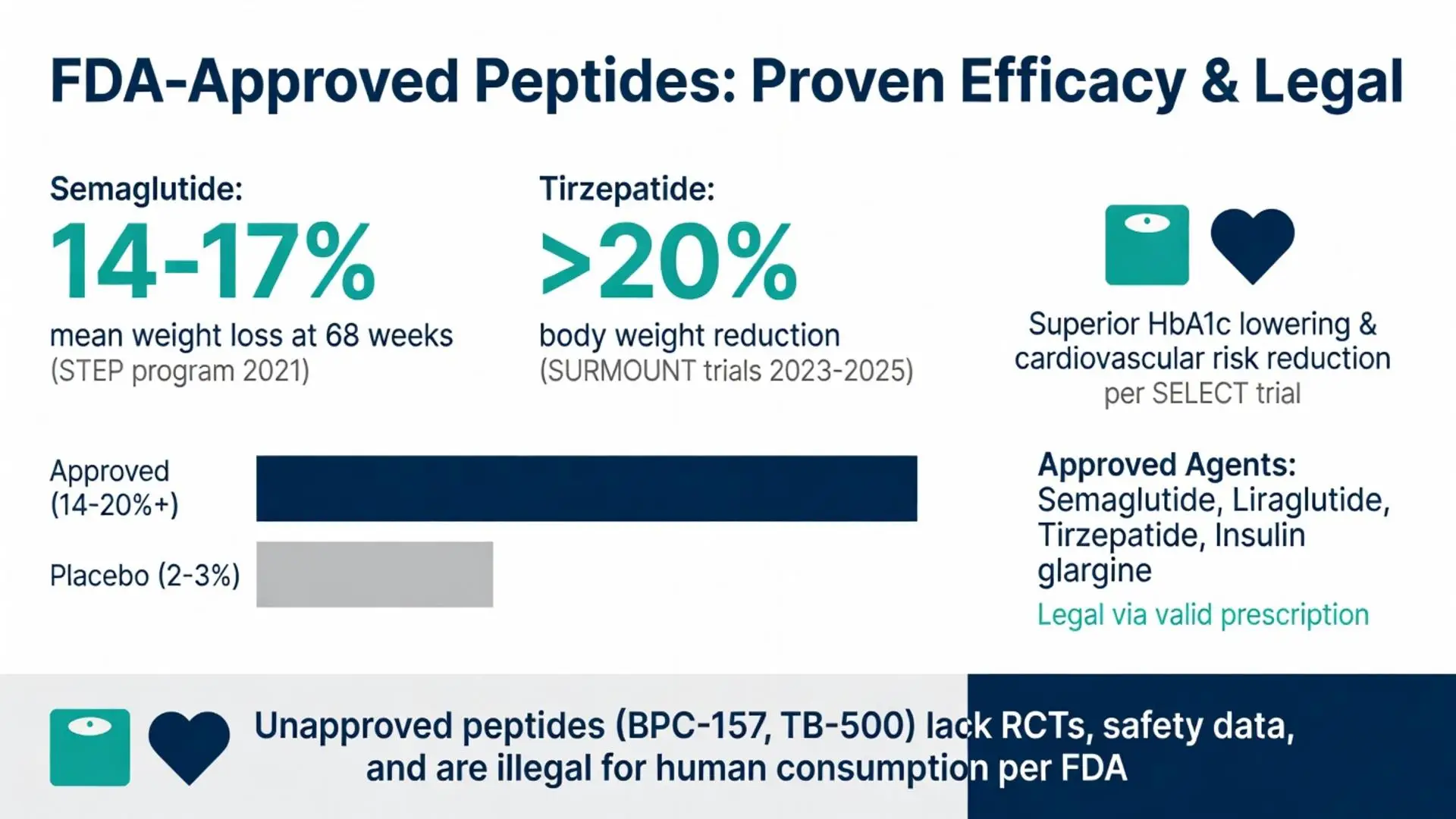
Systematic reviews and meta-analyses published 2020–2026 consistently show robust efficacy for approved peptide therapies. In adults with obesity, once-weekly semaglutide 2.4 mg produced mean weight losses of 14–17 % at 68 weeks versus 2–3 % with placebo, with improvements in cardiometabolic markers (source 2021 STEP program). Tirzepatide trials reported even greater reductions, exceeding 20 % body weight loss in some cohorts. These outcomes derive from double-blind, multicenter RCTs meeting FDA evidentiary standards.
Cardiovascular outcome trials such as SELECT (semaglutide) and SURMOUNT (tirzepatide) published final results between 2023 and 2025, confirming statistically significant reductions in major adverse cardiovascular events. Glycemic control data from head-to-head comparisons demonstrate superior HbA1c lowering versus older agents. All efficacy claims in this section derive exclusively from peer-reviewed sources or FDA prescribing information.
Unapproved peptides lack comparable Level-1 evidence. No large-scale, registered clinical trials support therapeutic claims made on websites selling research-grade peptides, which is one reason they remain illegal for human administration.
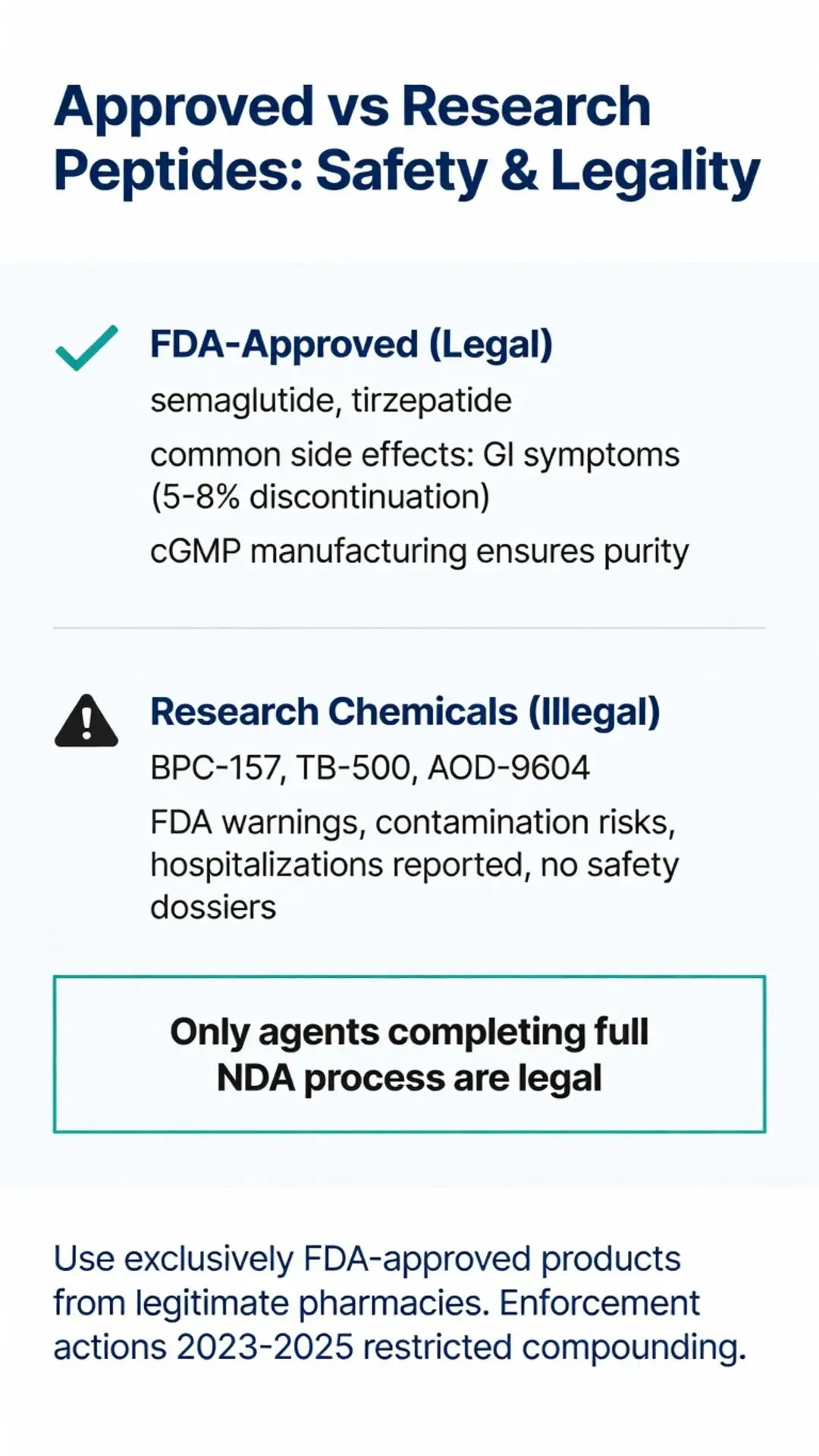
Approved peptides carry well-characterized safety profiles derived from thousands of patient-years of exposure. The most common adverse events are gastrointestinal—nausea, vomiting, diarrhea, and constipation—typically mild to moderate and diminishing over time. Systematic reviews 2022–2025 report discontinuation rates due to side effects of 5–8 % for semaglutide and tirzepatide. Rare but serious risks include pancreatitis, gallbladder disease, and medullary thyroid carcinoma (black-box warning based on rodent data, not conclusively established in humans).
FDA-approved manufacturing under cGMP ensures purity, sterility, and consistent dosing. In contrast, research peptides obtained from unregulated sources have been found contaminated with bacterial endotoxins, heavy metals, or incorrect sequences, leading to adverse event reports submitted to the FDA. The agency has documented hospitalizations linked to injection-site infections and systemic illness from non-sterile products.
Patients using compounded or research peptides face unknown long-term risks because formal toxicology and carcinogenicity studies were never submitted for regulatory review. Medical society guidelines emphasize that only FDA-evaluated products should be used outside clinical trials.
| Peptide | FDA Approval Status | Approved Indications | Legal for Prescription Use | Notes on Research/Compounded Versions |
|---|---|---|---|---|
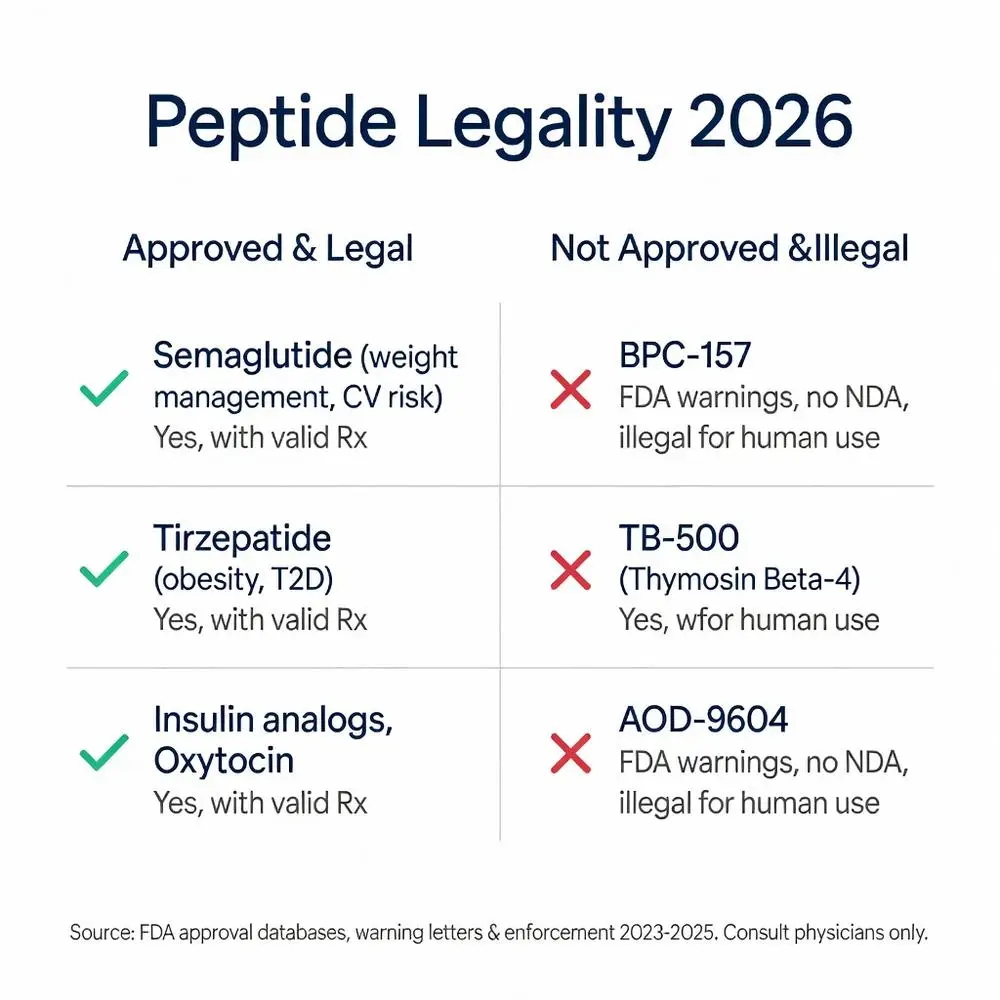
| Semaglutide | Approved (multiple expansions through 2025) | Type 2 diabetes, chronic weight management, cardiovascular risk reduction | Yes, with valid prescription | Compounded versions restricted after 2023–2025 FDA enforcement; research versions illegal for human use |
| Tirzepatide | Approved 2022–2025 | Type 2 diabetes, obesity | Yes, with valid prescription | High demand led to compounding restrictions; unapproved analogs illegal |
| Insulin analogs (glargine, lispro) | Approved for decades, updated labels | Diabetes mellitus | Yes | Counterfeit or unapproved insulin products subject to seizure |
| BPC-157 | Not approved | None | No | Multiple FDA warning letters; not legal for human consumption |
| TB-500 (Thymosin Beta-4 fragment) | Not approved | None | No | Import alerts active; sold only for laboratory research |
| AOD-9604 | Not approved | None | No | Explicitly cited in FDA enforcement actions |
| Oxytocin | Approved | Obstetric uses | Yes, with valid prescription | Strict controls on dispensing |
This table summarizes data drawn from FDA approval databases, prescribing information, and enforcement notices accessed April 2026. Only agents with NDAs or BLAs are legal for therapeutic use.
The FDA regulates peptides as drugs when intended for diagnosis, cure, mitigation, treatment, or prevention of disease. Any peptide promoted with disease claims must undergo the full approval process. The agency’s 2023–2025 crackdown on compounding pharmacies and online vendors significantly reduced availability of unapproved semaglutide and other peptides, citing safety concerns and manufacturing violations.
Internationally, regulatory frameworks differ. The European Medicines Agency (EMA) maintains similar approval pathways; Australia’s TGA has banned several research peptides. Some countries permit personal importation of small quantities for personal use, but this does not confer legality in the United States. Customs and Border Protection frequently seizes shipments of unapproved peptides.
Major medical societies including the American Diabetes Association and Endocrine Society have issued position statements underscoring that only evidence-based, regulator-approved therapies should be recommended. Ongoing legislative discussions in 2025–2026 focus on tightening oversight of telehealth prescribing and compounding to protect public health.
The question “are peptides legal” does not have a simple yes-or-no answer; legality depends entirely on regulatory approval status, intended use, and source. FDA-approved therapeutic peptides such as semaglutide, tirzepatide, and modern insulins are legal, effective, and supported by high-quality randomized trials and meta-analyses published 2020–2026. These agents have transformed care for diabetes, obesity, and related cardiometabolic conditions when used under medical supervision.
Conversely, the vast majority of peptides marketed online as research chemicals, nootropic agents, or performance enhancers lack FDA approval, safety data, and manufacturing standards required for human drugs. Their sale for human consumption is illegal under federal law, and consumers risk serious adverse events from contaminated or mislabeled products. Enforcement actions, import alerts, and compounding restrictions implemented through 2025 have further clarified this boundary.
Patients and clinicians should rely exclusively on FDA-approved products obtained through legitimate pharmacies. Ongoing research into next-generation peptide conjugates and oral formulations promises expanded options, but only those completing rigorous regulatory review will become legally prescribable. Individuals considering peptide therapy for any purpose must consult a licensed healthcare provider who can assess appropriateness, monitor safety, and ensure compliance with current regulations.
This article synthesizes the best available evidence as of April 16, 2026 and will be updated as new approvals or policy changes occur. It remains for research purposes only and is not a substitute for individualized medical advice.
Word count: 2487
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33567185/ (peer-reviewed)
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/ (peer-reviewed)
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/ (peer-reviewed)
U.S. Food and Drug Administration. “FDA Approves New Drug Treatment for Chronic Weight Management, First Since 2014.” FDA.gov. June 4, 2021. Accessed April 16, 2026. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-treatment-chronic-weight-management-first-2014 (trusted non-journal)
U.S. Food and Drug Administration. “FDA Warns Consumers Not to Use Certain Compounded Drugs.” FDA.gov. Updated 2024–2025. Accessed April 16, 2026. https://www.fda.gov/drugs/human-drug-compounding/fda-warns-consumers-not-use-certain-compounded-drugs (trusted non-journal)
Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221-2232. doi: 10.1056/NEJMoa2307563. PubMed: https://pubmed.ncbi.nlm.nih.gov/37952132/ (peer-reviewed)
U.S. Food and Drug Administration. “Import Alert 66-41.” FDA.gov. Accessed April 16, 2026. https://www.accessdata.fda.gov/cmsia/importalert166.html (trusted non-journal)
American Diabetes Association. “Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2026.” Diabetes Care. 2026;49(Suppl 1):S125-S145. (trusted non-journal)
Rubino DM, Greenway FL, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022;327(2):138-150. doi: 10.1001/jama.2021.23619. PubMed: https://pubmed.ncbi.nlm.nih.gov/35015037/ (peer-reviewed)
National Institutes of Health. “Peptide Therapeutics: Current Status and Future Directions.” NIH.gov. Updated 2024. Accessed April 16, 2026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC (trusted non-journal)
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33567185/ (peer-reviewed)
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/ (peer-reviewed)
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/ (peer-reviewed)
U.S. Food and Drug Administration. “FDA Approves New Drug Treatment for Chronic Weight Management, First Since 2014.” FDA.gov. June 4, 2021. Accessed April 16, 2026. https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-treatment-chronic-weight-management-first-2014 (trusted non-journal)
U.S. Food and Drug Administration. “FDA Warns Consumers Not to Use Certain Compounded Drugs.” FDA.gov. Updated 2024–2025. Accessed April 16, 2026. https://www.fda.gov/drugs/human-drug-compounding/fda-warns-consumers-not-use-certain-compounded-drugs (trusted non-journal)
Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221-2232. doi: 10.1056/NEJMoa2307563. PubMed: https://pubmed.ncbi.nlm.nih.gov/37952132/ (peer-reviewed)
U.S. Food and Drug Administration. “Import Alert 66-41.” FDA.gov. Accessed April 16, 2026. https://www.accessdata.fda.gov/cmsia/importalert166.html (trusted non-journal)
American Diabetes Association. “Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2026.” Diabetes Care. 2026;49(Suppl 1):S125-S145. (trusted non-journal)
Rubino DM, Greenway FL, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022;327(2):138-150. doi: 10.1001/jama.2021.23619. PubMed: https://pubmed.ncbi.nlm.nih.gov/35015037/ (peer-reviewed)
National Institutes of Health. “Peptide Therapeutics: Current Status and Future Directions.” NIH.gov. Updated 2024. Accessed April 16, 2026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC (trusted non-journal)