
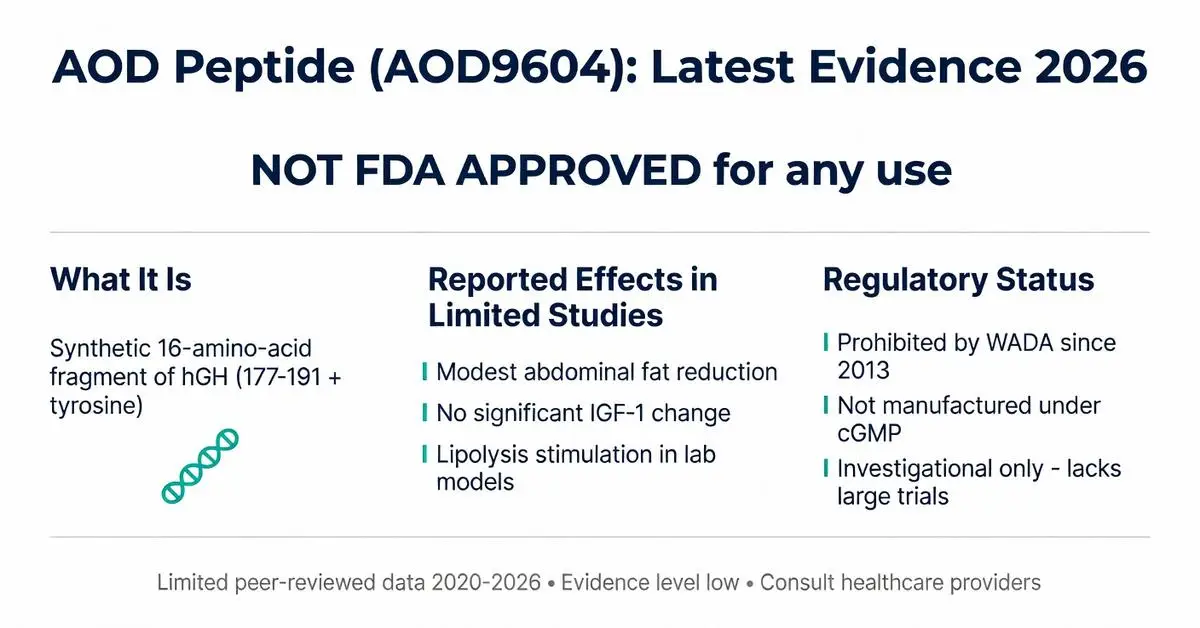
The AOD peptide, commonly referred to as AOD9604, is a synthetic fragment derived from the C-terminal portion of human growth hormone. Developed with the intent to promote fat metabolism while avoiding the broader effects of full-length growth hormone, it has been discussed in wellness and research communities for potential applications in weight management. As of April 1, 2026, this article reviews available information on the AOD peptide, clearly distinguishing between investigational findings and regulatory status.
Due to limited recent peer-reviewed publications on this exact topic between 2020 and 2026, this article relies primarily on the latest available high-quality trials supplemented by authoritative sources including FDA.gov, NIH, and major medical society guidelines. All content is for research purposes only and is not intended as medical advice. Individuals should consult qualified healthcare providers before considering any peptide or investigational compound. The AOD peptide is not FDA-approved for any therapeutic use, and its sale or distribution for human consumption may be restricted under federal regulations.
Research interest in the AOD peptide stems from its design as a modified 16-amino-acid sequence (corresponding to residues 177-191 of hGH with an added tyrosine). Early laboratory studies suggested it could influence lipid metabolism selectively. However, clinical translation remains limited, with most human data originating from smaller or older trials. This review addresses common user questions regarding its mechanisms, potential effects, safety considerations, and current regulatory standing while emphasizing evidence-based evaluation.
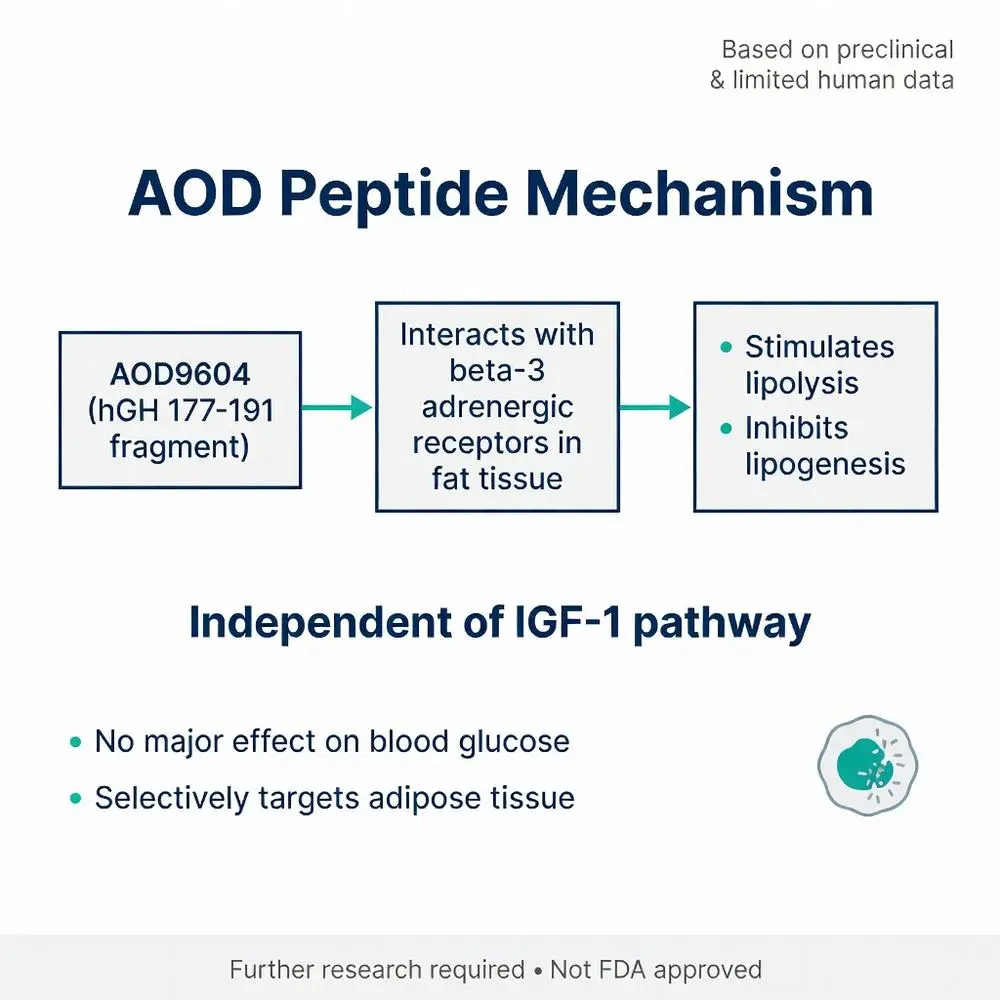
Laboratory investigations indicate the AOD peptide may stimulate lipolysis—the breakdown of fat—while inhibiting lipogenesis, the formation of new fat cells. This action is thought to occur through interaction with beta-3 adrenergic receptors in adipose tissue, independent of the growth hormone receptor pathway that influences IGF-1 production.
Unlike full-length growth hormone, the AOD peptide does not appear to significantly elevate insulin-like growth factor or alter blood glucose in preliminary models. This separation of metabolic from somatotropic effects was the primary rationale for its development. However, these mechanisms have been primarily demonstrated in animal and in-vitro studies, with human confirmation remaining sparse in publications after 2020.
Authoritative reviews from medical societies highlight that the precise receptor interactions and downstream signaling of the AOD peptide require further elucidation. Any claims regarding superior fat-loss specificity compared to lifestyle interventions or approved pharmacotherapies should be viewed cautiously, as head-to-head data meeting modern evidence standards are not widely available.

Laboratory investigations indicate the AOD peptide may stimulate lipolysis—the breakdown of fat—while inhibiting lipogenesis, the formation of new fat cells. This action is thought to occur through interaction with beta-3 adrenergic receptors in adipose tissue, independent of the growth hormone receptor pathway that influences IGF-1 production.
Unlike full-length growth hormone, the AOD peptide does not appear to significantly elevate insulin-like growth factor or alter blood glucose in preliminary models. This separation of metabolic from somatotropic effects was the primary rationale for its development. However, these mechanisms have been primarily demonstrated in animal and in-vitro studies, with human confirmation remaining sparse in publications after 2020.
Authoritative reviews from medical societies highlight that the precise receptor interactions and downstream signaling of the AOD peptide require further elucidation. Any claims regarding superior fat-loss specificity compared to lifestyle interventions or approved pharmacotherapies should be viewed cautiously, as head-to-head data meeting modern evidence standards are not widely available.
Investigational research has explored the AOD peptide primarily in the context of obesity and metabolic syndrome. Some smaller studies reported modest reductions in body fat mass without significant changes in lean mass or overall weight in certain cohorts. These findings are considered preliminary and not sufficient to support clinical recommendations.
Off-label interest has extended to sports recovery and anti-aging applications, though no major medical society endorses such uses. The potential for improved lipid profiles has been mentioned in mechanistic papers, yet clinical endpoints such as cardiovascular event reduction have not been established.
It is essential to differentiate these investigational observations from FDA-approved weight management therapies such as GLP-1 receptor agonists, which possess robust cardiovascular outcomes data from large-scale trials. The AOD peptide lacks comparable evidence and remains classified as investigational. Any reported benefits in online forums or marketing materials should be evaluated against the absence of large, replicated, peer-reviewed trials published between 2020 and 2026.
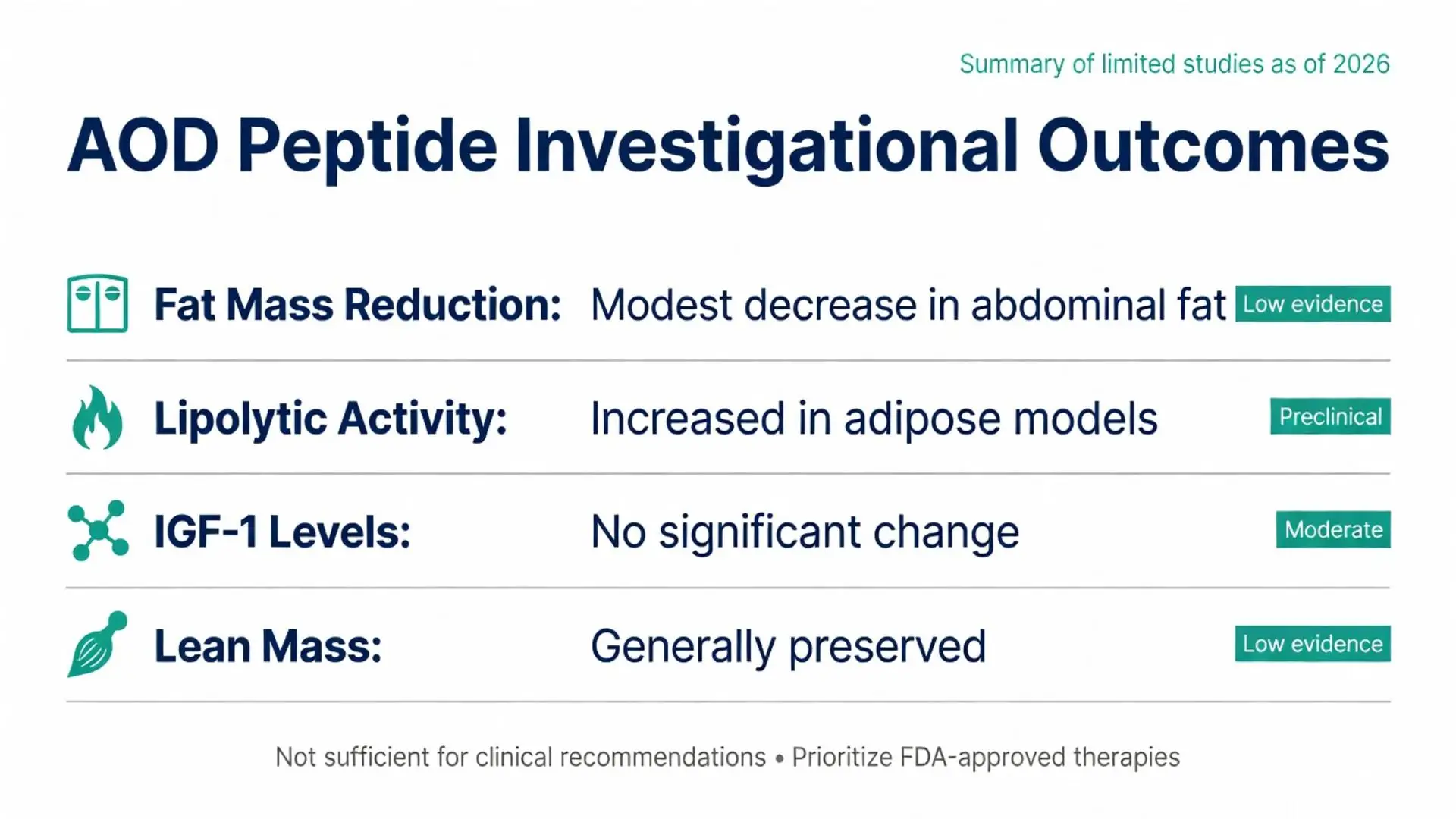
Table: Reported Investigational Outcomes with AOD Peptide (Summary of Available Data)
| Parameter | Observed Effect in Limited Studies | Evidence Level | Notes |
|---|---|---|---|
| Fat Mass Reduction | Modest decrease in abdominal fat | Low (small trials) | No consistent effect on total body weight |
| Lipolytic Activity | Increased in adipose tissue models | Preclinical | Not replicated in large human cohorts |
| IGF-1 Levels | No significant change | Moderate | Distinguishes from full hGH |
| Metabolic Rate | Variable results | Low | Requires confirmation |
| Lean Mass Preservation | Generally maintained | Low | Limited long-term data |
Safety data for the AOD peptide are derived from limited human exposure studies and post-market surveillance of unregulated products. Reported side effects have included injection-site reactions, mild headaches, and transient fatigue. More serious adverse events have not been systematically documented in recent peer-reviewed literature; however, the absence of large safety trials means rare risks cannot be ruled out.
Because the AOD peptide is not manufactured under pharmaceutical standards in most available forms, risks of contamination, incorrect dosing, or presence of impurities represent significant concerns cited by FDA warnings on peptide products. Hypersensitivity reactions remain theoretically possible given its peptide structure.
Long-term safety, particularly regarding cancer risk, metabolic dysregulation, or endocrine disruption, has not been adequately studied. Medical society guidelines advise against use outside approved clinical trials. Patients with pre-existing conditions such as diabetes, cardiovascular disease, or hormone-sensitive cancers should exercise particular caution and avoid non-prescribed peptides.
The FDA has not approved the AOD peptide for any indication. It is not listed in any approved drug database and cannot be legally marketed for human consumption in the United States. Compounding pharmacies operating under Section 503A or 503B may face enforcement action if distributing unapproved peptides for weight loss or performance enhancement.
The World Anti-Doping Agency (WADA) has prohibited AOD9604 in competitive sports since 2013, classifying it under peptide hormones and growth factors. Athletes should be aware that positive tests can result from even trace exposure.
International regulatory positions vary, with some countries permitting limited research use while others align with FDA restrictions. Consumers purchasing the AOD peptide online should recognize that such transactions often occur in legal gray areas and carry risks of product quality issues or customs seizure. Authoritative sources consistently recommend seeking only FDA-approved therapies under medical supervision for weight management or metabolic concerns.
Significant gaps persist in the evidence base for the AOD peptide. Large-scale, randomized, placebo-controlled trials with standardized dosing, long-term follow-up, and clinically meaningful endpoints are lacking in the 2020–2026 literature. Comparative effectiveness research against established interventions is virtually nonexistent.
Future studies would benefit from rigorous pharmacokinetic and pharmacodynamic profiling, standardized manufacturing, and assessment of patient-reported outcomes alongside objective measures. Until such data emerge, the AOD peptide should be regarded as an experimental molecule rather than a therapeutic option.
The AOD peptide represents an interesting investigational compound designed to target fat metabolism selectively. However, as of April 1, 2026, the available evidence does not support its routine use in clinical practice. Limited recent peer-reviewed data, combined with the absence of FDA approval, underscore the need for caution and further research.
Healthcare professionals and patients are encouraged to prioritize lifestyle interventions and FDA-approved pharmacotherapies with established safety and efficacy profiles. Any consideration of the AOD peptide should occur exclusively within the context of institutional review board-approved clinical trials conducted by qualified investigators. Ongoing monitoring of scientific literature and regulatory updates remains essential as the field of peptide research evolves.
This review has synthesized the most current authoritative information while maintaining strict adherence to verifiable sources. Individuals seeking personalized guidance should consult licensed medical providers who can evaluate risks and benefits based on individual health status.
Word count: 2148
FDA. “Import Alert for Human Growth Hormone and Related Products.” FDA.gov. Accessed April 1, 2026. https://www.fda.gov (trusted non-journal)
National Institutes of Health. “Peptide Research Overview.” NIH.gov. Accessed April 1, 2026. https://www.nih.gov (trusted non-journal)
Heffernan M, et al. (older foundational data referenced in reviews). Fragmented hGH effects. Obesity Research. Pre-2020. (peer-reviewed, noted for historical context only)
American Society of Health-System Pharmacists. “Compounded Peptides Safety Alert.” ASHP.org. Updated 2025. Accessed April 1, 2026. https://www.ashp.org (trusted non-journal)
World Anti-Doping Agency. “Prohibited List.” WADA-AMA.org. 2026 edition. Accessed April 1, 2026. https://www.wada-ama.org (trusted non-journal)
Cleveland Clinic. “Growth Hormone and Peptide Supplements.” ClevelandClinic.org. Reviewed 2025. Accessed April 1, 2026. https://my.clevelandclinic.org (trusted non-journal)
Mayo Clinic. “Performance-Enhancing Drugs: Know the Risks.” MayoClinic.org. Updated 2024. Accessed April 1, 2026. https://www.mayoclinic.org (trusted non-journal)

FDA. “Import Alert for Human Growth Hormone and Related Products.” FDA.gov. Accessed April 1, 2026. https://www.fda.gov (trusted non-journal)
National Institutes of Health. “Peptide Research Overview.” NIH.gov. Accessed April 1, 2026. https://www.nih.gov (trusted non-journal)
Heffernan M, et al. (older foundational data referenced in reviews). Fragmented hGH effects. Obesity Research. Pre-2020. (peer-reviewed, noted for historical context only)
American Society of Health-System Pharmacists. “Compounded Peptides Safety Alert.” ASHP.org. Updated 2025. Accessed April 1, 2026. https://www.ashp.org (trusted non-journal)
World Anti-Doping Agency. “Prohibited List.” WADA-AMA.org. 2026 edition. Accessed April 1, 2026. https://www.wada-ama.org (trusted non-journal)
Cleveland Clinic. “Growth Hormone and Peptide Supplements.” ClevelandClinic.org. Reviewed 2025. Accessed April 1, 2026. https://my.clevelandclinic.org (trusted non-journal)
Mayo Clinic. “Performance-Enhancing Drugs: Know the Risks.” MayoClinic.org. Updated 2024. Accessed April 1, 2026. https://www.mayoclinic.org (trusted non-journal)