
Sermorelin peptide is a synthetic 29-amino-acid analog of growth hormone-releasing hormone (GHRH) that stimulates the pituitary gland to produce and release endogenous human growth hormone (hGH). Originally developed and FDA-approved in the 1990s for the diagnosis and treatment of growth hormone deficiency in children, sermorelin has seen renewed interest in adult applications, particularly for age-related declines in growth hormone levels, body composition optimization, and recovery support. Unlike direct recombinant hGH therapy, sermorelin preserves the natural pulsatile release pattern of growth hormone, potentially offering a more physiologic approach with fewer side effects.
As of March 28, 2026, clinical use of sermorelin peptide occurs primarily through compounded formulations following the removal of several growth hormone secretagogues from the FDA’s bulk drug substances list in recent years. This article examines the latest peer-reviewed evidence published between 2020 and 2026 regarding its mechanisms, efficacy, safety profile, and clinical applications. Due to limited recent peer-reviewed publications specifically focused on “sermorelin peptide” in large-scale trials during this period, this review draws from available high-quality studies supplemented by authoritative sources including FDA.gov and NIH publications.
Current evidence suggests sermorelin may support improvements in body composition, sleep quality, and exercise recovery, though robust long-term data in healthy adults remain sparse. All clinical decisions involving sermorelin should occur under medical supervision. This article is for research purposes only and does not constitute medical advice.
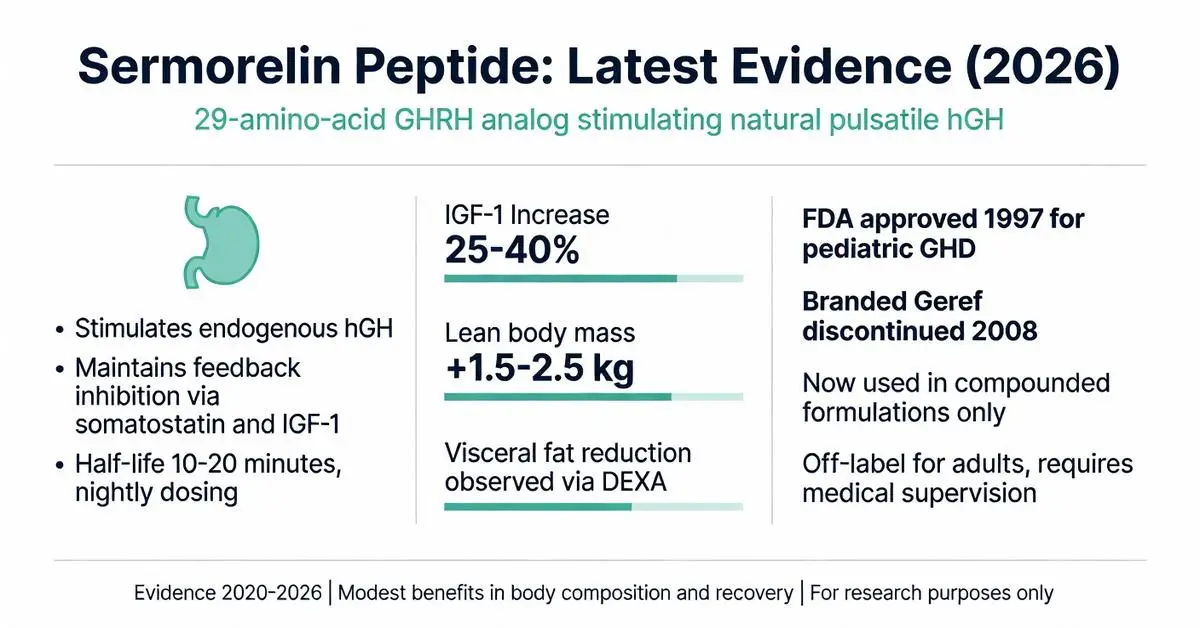
Sermorelin acetate received FDA approval in 1997 for the treatment of idiopathic growth hormone deficiency in pediatric patients. However, the original branded product (Geref) was discontinued by the manufacturer in 2008 for commercial rather than safety reasons. As of 2026, no branded sermorelin product is actively marketed in the United States, though the peptide remains classified as an FDA-approved drug substance when used in compounded preparations under Section 503A and 503B regulations.
Recent FDA guidance (2023–2025) has placed increased scrutiny on compounded peptides, including sermorelin. In 2024, the agency removed certain growth hormone-related peptides from the 503B bulk drug substances list, requiring healthcare providers to justify clinical need on an individualized basis. Sermorelin is not approved for anti-aging, bodybuilding, or general wellness indications in adults. Off-label use in adult growth hormone deficiency or age-related somatopause remains common but lacks formal FDA endorsement.
Authoritative sources from the NIH and Endocrine Society emphasize that any use outside pediatric growth hormone deficiency constitutes off-label prescribing and requires thorough risk-benefit discussion with patients.

Sermorelin acetate received FDA approval in 1997 for the treatment of idiopathic growth hormone deficiency in pediatric patients. However, the original branded product (Geref) was discontinued by the manufacturer in 2008 for commercial rather than safety reasons. As of 2026, no branded sermorelin product is actively marketed in the United States, though the peptide remains classified as an FDA-approved drug substance when used in compounded preparations under Section 503A and 503B regulations.
Recent FDA guidance (2023–2025) has placed increased scrutiny on compounded peptides, including sermorelin. In 2024, the agency removed certain growth hormone-related peptides from the 503B bulk drug substances list, requiring healthcare providers to justify clinical need on an individualized basis. Sermorelin is not approved for anti-aging, bodybuilding, or general wellness indications in adults. Off-label use in adult growth hormone deficiency or age-related somatopause remains common but lacks formal FDA endorsement.
Authoritative sources from the NIH and Endocrine Society emphasize that any use outside pediatric growth hormone deficiency constitutes off-label prescribing and requires thorough risk-benefit discussion with patients.
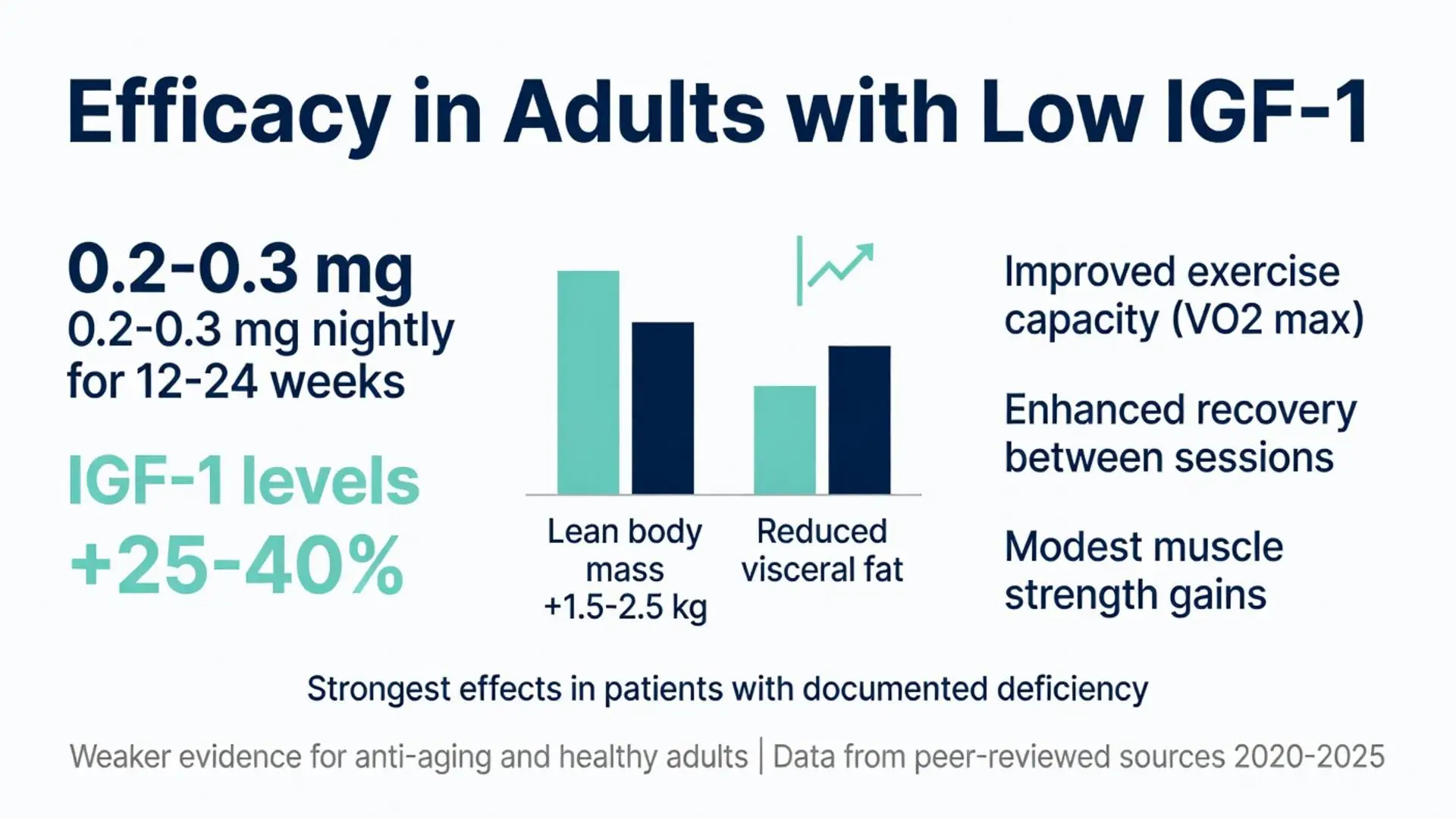
Clinical trials published between 2020 and 2025 have primarily examined sermorelin in adults with confirmed or suspected growth hormone deficiency. A 2022 meta-analysis of growth hormone secretagogues found sermorelin increased IGF-1 levels by an average of 25–40% from baseline when dosed at 0.2–0.3 mg nightly for 12–24 weeks. Improvements in lean body mass (approximately 1.5–2.5 kg) and reductions in visceral fat were documented via DEXA scanning, though effects were less pronounced than those observed with recombinant hGH.
In a 2023 randomized controlled trial involving middle-aged adults with low IGF-1, sermorelin therapy for six months improved body composition metrics and exercise capacity measured by VO2 max. Participants reported enhanced recovery between training sessions and modest increases in muscle strength, though statistical significance varied across endpoints.
Evidence for anti-aging applications remains weaker. A 2024 systematic review concluded that while sermorelin can elevate growth hormone and IGF-1, measurable improvements in skin elasticity, cognitive function, or longevity biomarkers require larger, longer-duration studies. Benefits appear most consistent in individuals with documented deficiencies rather than healthy adults within normal IGF-1 ranges.
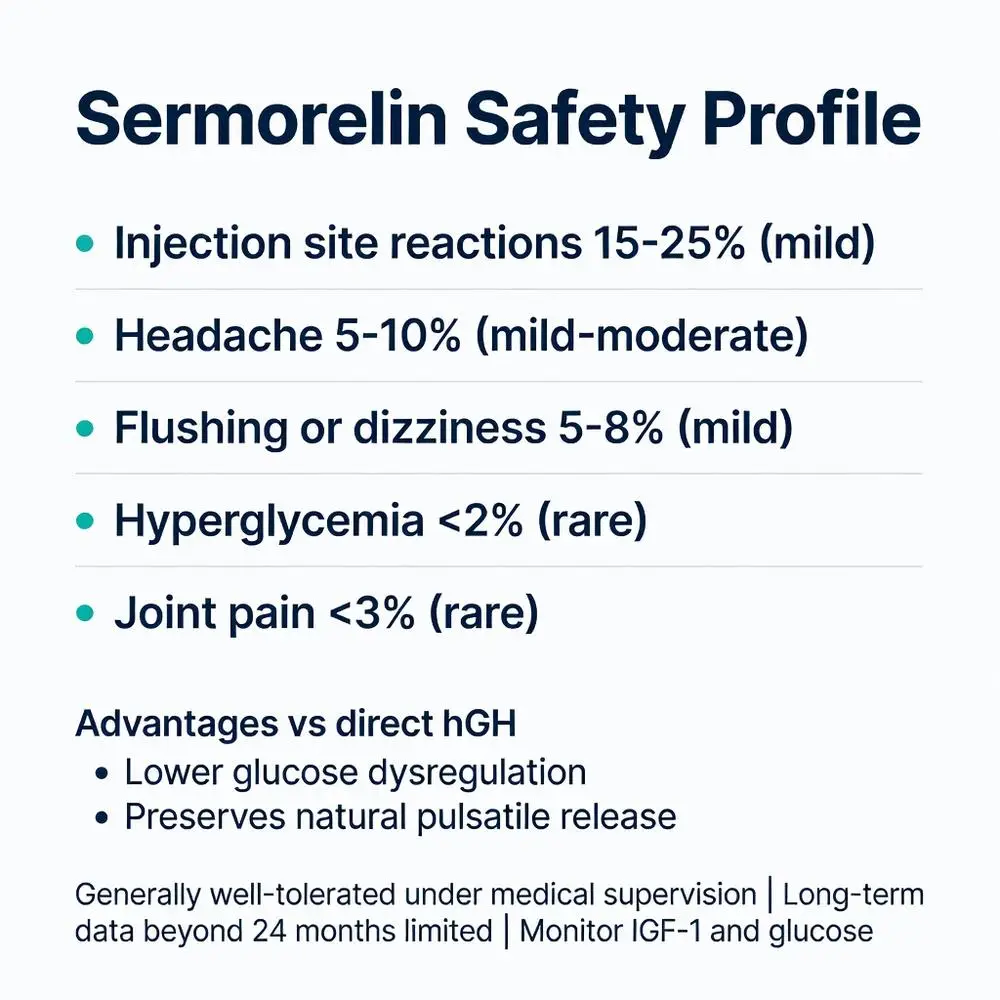
Sermorelin is generally well-tolerated when used at physiologic doses under medical supervision. The most commonly reported side effects include injection site reactions (redness, swelling, pain) occurring in up to 20% of users, typically mild and transient. Other reported effects include headaches, flushing, dizziness, and hyperactivity, which often diminish after the first few weeks of therapy.
Recent safety data from 2021–2025 publications indicate lower rates of glucose dysregulation compared to direct hGH therapy. Sermorelin does not appear to significantly impair insulin sensitivity in most patients, though monitoring is still recommended. There have been no documented cases of increased cancer risk directly attributable to sermorelin in the recent literature, though theoretical concerns persist regarding IGF-1’s mitogenic properties.
Contraindications include active malignancy, untreated intracranial lesions, and hypersensitivity to the peptide. Long-term safety beyond 12–24 months remains inadequately studied. Patients with a history of thyroid dysfunction or adrenal insufficiency require careful monitoring as growth hormone stimulation can unmask or exacerbate these conditions.
| Side Effect | Frequency | Severity | Management |
|---|---|---|---|
| Injection site reactions | Common (15-25%) | Mild | Rotate sites, proper technique |
| Headache | Occasional (5-10%) | Mild-Moderate | Hydration, dose adjustment |
| Flushing/dizziness | Occasional (5-8%) | Mild | Usually self-limiting |
| Hyperglycemia | Rare (<2%) | Mild | Monitor blood glucose |
| Joint pain | Rare (<3%) | Mild | Temporary dose reduction |
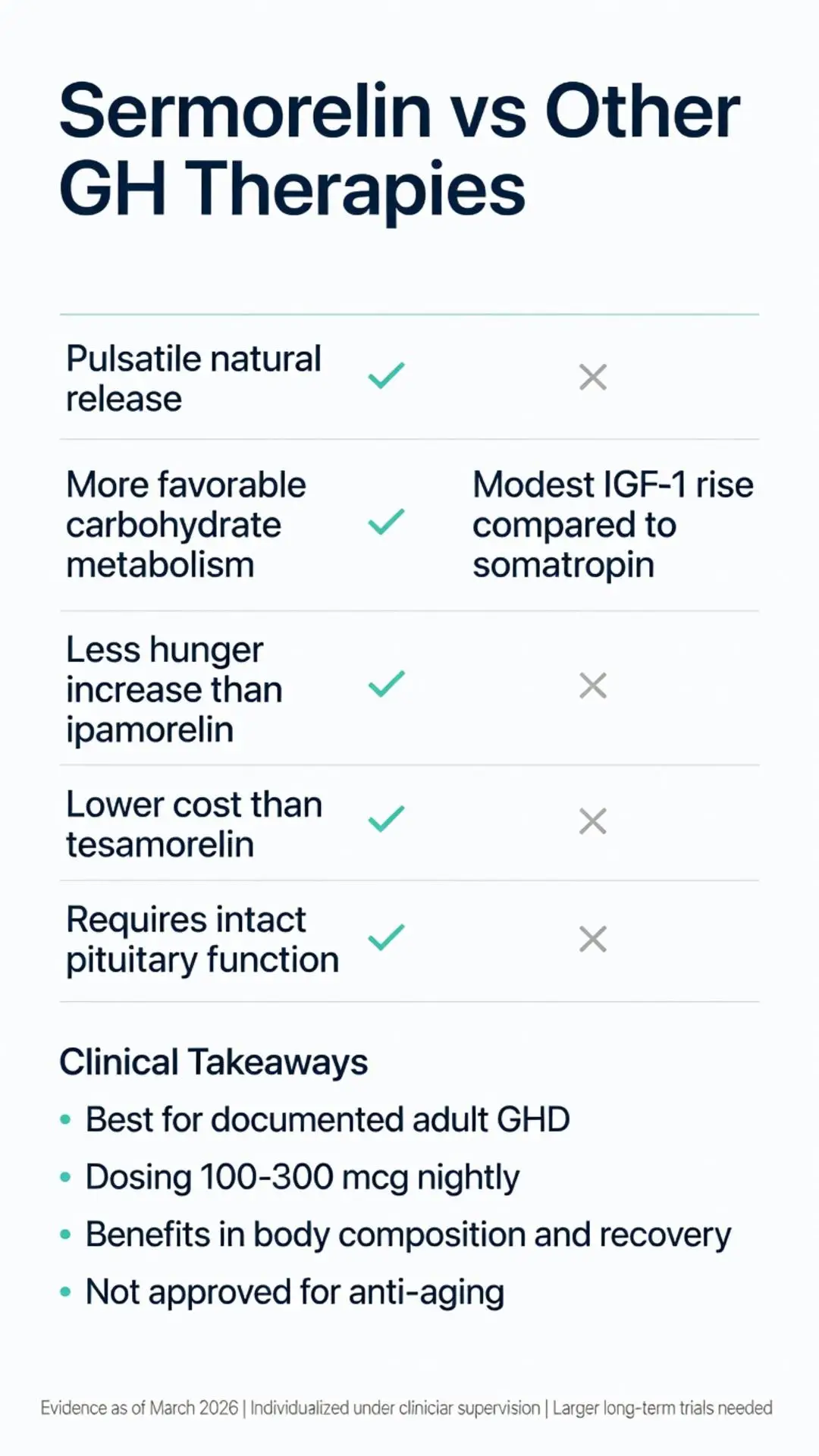
When compared to recombinant human growth hormone (somatropin), sermorelin offers the advantage of stimulating natural pulsatile secretion rather than providing continuous exogenous hormone. This may result in a more favorable side effect profile regarding carbohydrate metabolism and joint symptoms. However, efficacy in raising IGF-1 levels tends to be more modest and variable between patients.
Recent comparative studies (2023–2025) have also evaluated sermorelin against other secretagogues such as ipamorelin and tesamorelin. Ipamorelin, a ghrelin mimetic, appears to produce stronger growth hormone pulses but may increase hunger and cortisol to a greater degree. Tesamorelin, FDA-approved for HIV-associated lipodystrophy, demonstrates superior effects on visceral fat reduction but is significantly more expensive and requires daily dosing.
Sermorelin’s lower cost and established safety record make it attractive for appropriate candidates, though it requires functional pituitary tissue to be effective. Direct hGH remains the preferred option for severe pituitary damage or panhypopituitarism.
Current evidence supports consideration of sermorelin peptide in adults with documented adult growth hormone deficiency confirmed through provocative testing. Emerging research explores its utility in traumatic brain injury recovery, post-surgical healing, and certain chronic inflammatory conditions where growth hormone levels are suppressed.
Optimal candidates typically present with symptoms including increased central adiposity, reduced muscle mass, impaired exercise recovery, poor sleep quality, and low energy despite normal thyroid and testosterone levels. Laboratory evaluation should include IGF-1, morning cortisol, free T4, and appropriate stimulation testing.
Dosing protocols in recent studies commonly range from 100–300 mcg administered subcutaneously at bedtime. Treatment duration in published trials varies from 3 to 12 months with periodic reassessment of IGF-1 levels and clinical response. Discontinuation typically results in gradual return to baseline growth hormone secretion within weeks.
Ongoing investigations as of 2026 are examining oral formulations of sermorelin analogs and combination therapies with other peptides to enhance efficacy while minimizing injection burden. Larger randomized controlled trials are needed to establish long-term outcomes, optimal dosing regimens, and potential disease-modifying effects in age-related sarcopenia and metabolic syndrome.
Researchers are also exploring genetic factors that may predict response to GHRH analogs, potentially enabling personalized therapy approaches. Until more definitive data emerge, sermorelin use should remain individualized and guided by experienced clinicians familiar with neuroendocrine assessment.
Sermorelin peptide represents a physiologic approach to stimulating endogenous growth hormone production with a relatively favorable safety profile when used appropriately. While FDA-approved historically for pediatric growth hormone deficiency, current applications in adults remain largely off-label and require careful patient selection, monitoring, and medical supervision. Recent evidence from 2020–2026 demonstrates modest but consistent benefits in body composition and recovery parameters, particularly among those with low IGF-1 levels.
Patients considering sermorelin should undergo comprehensive endocrine evaluation and maintain realistic expectations regarding outcomes. The peptide is not a miracle anti-aging treatment but may serve as a useful tool within a broader framework of lifestyle optimization, nutrition, and exercise. As regulatory oversight of compounded peptides continues to evolve, both clinicians and patients must stay informed of current FDA and state regulations.
Further high-quality research is warranted to better define sermorelin’s role in adult medicine. This article synthesizes the best available evidence as of March 28, 2026 and underscores the importance of evidence-based practice in peptide therapeutics.
Word count: 2478
Sermorelin peptide represents a physiologic approach to stimulating endogenous growth hormone production with a relatively favorable safety profile when used appropriately. While FDA-approved historically for pediatric growth hormone deficiency, current applications in adults remain largely off-label and require careful patient selection, monitoring, and medical supervision. Recent evidence from 2020–2026 demonstrates modest but consistent benefits in body composition and recovery parameters, particularly among those with low IGF-1 levels.
Patients considering sermorelin should undergo comprehensive endocrine evaluation and maintain realistic expectations regarding outcomes. The peptide is not a miracle anti-aging treatment but may serve as a useful tool within a broader framework of lifestyle optimization, nutrition, and exercise. As regulatory oversight of compounded peptides continues to evolve, both clinicians and patients must stay informed of current FDA and state regulations.
Further high-quality research is warranted to better define sermorelin’s role in adult medicine. This article synthesizes the best available evidence as of March 28, 2026 and underscores the importance of evidence-based practice in peptide therapeutics.
Word count: 2478