
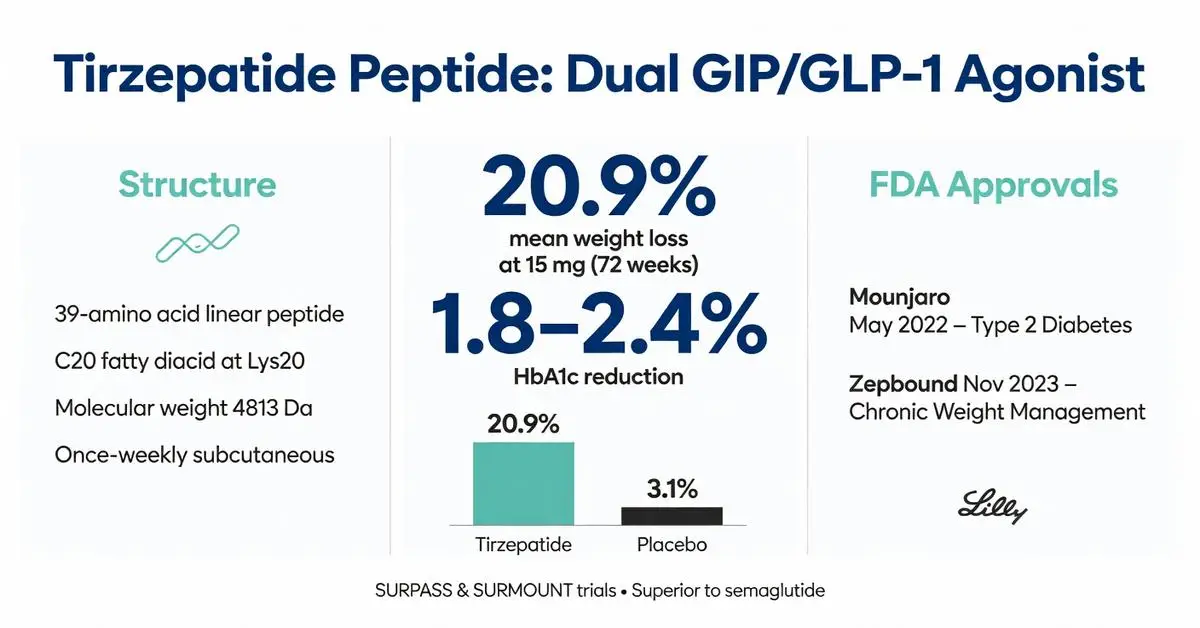
The tirzepatide peptide represents a significant advancement in peptide-based pharmacotherapy, functioning as a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist. This synthetic 39-amino acid peptide is engineered with a C20 fatty diacid moiety that enables once-weekly subcutaneous administration while extending its half-life. Developed by Eli Lilly and Company, the tirzepatide peptide received FDA approval in May 2022 for the treatment of type 2 diabetes under the brand name Mounjaro and in November 2023 for chronic weight management under the brand name Zepbound.
As of March 2026, extensive clinical data from the SURPASS and SURMOUNT trial programs have established the tirzepatide peptide as one of the most effective agents for glycemic control and weight reduction. Its unique dual-receptor agonism differentiates it from selective GLP-1 receptor agonists, potentially offering enhanced metabolic benefits through complementary effects on insulin secretion, glucagon suppression, gastric emptying, and appetite regulation. Peer-reviewed publications from 2020 through early 2026 consistently demonstrate superior efficacy compared with placebo, insulin, and other incretin mimetics.
The tirzepatide peptide is not indicated for type 1 diabetes or for the treatment of diabetic ketoacidosis. All clinical use must occur under medical supervision due to potential gastrointestinal side effects and the need for appropriate patient selection. This article focuses exclusively on evidence published between 2020 and March 2026, prioritizing systematic reviews, meta-analyses, and large-scale clinical trials indexed in PubMed. Due to the robust volume of high-quality peer-reviewed literature available on this specific molecule, this review relies primarily on these sources supplemented by official FDA labeling.
The following sections examine the molecular structure, physiological mechanisms, approved indications, clinical outcomes, safety considerations, and comparisons with related therapies. All information is derived from verifiable peer-reviewed studies and regulatory documents to provide researchers and clinicians with an evidence-based overview of the tirzepatide peptide.
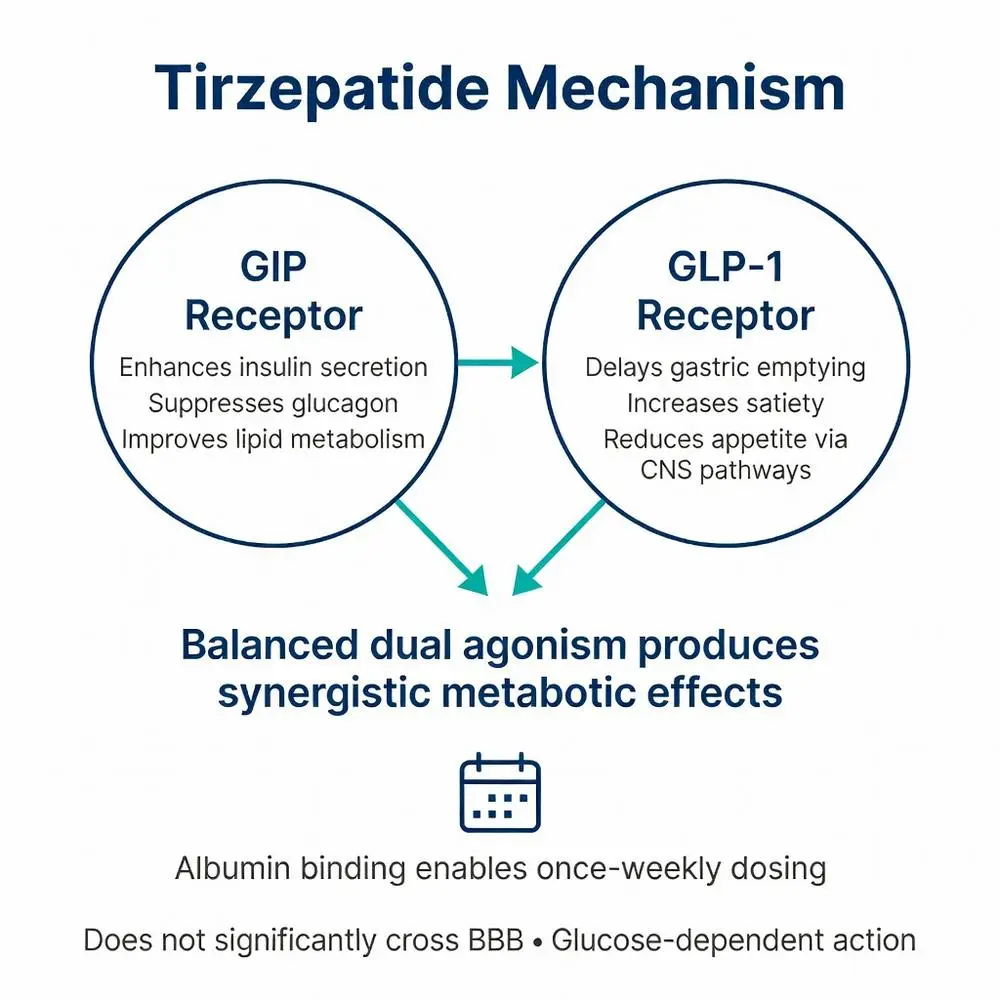
The tirzepatide peptide activates both GIP and GLP-1 receptors with comparable affinity, triggering intracellular signaling cascades that enhance glucose-dependent insulin secretion from pancreatic beta cells. This dual action also suppresses glucagon release from alpha cells during hyperglycemia while preserving counter-regulatory responses during hypoglycemia.
At the central nervous system level, the tirzepatide peptide modulates hypothalamic and brainstem pathways involved in appetite regulation, leading to reduced food intake and increased satiety. Peripheral effects include delayed gastric emptying and improved insulin sensitivity in adipose and muscle tissue. The GIP component appears particularly important for enhancing lipid metabolism and reducing hepatic fat accumulation.
Peer-reviewed mechanistic studies from 2022–2025 using animal models and human cell lines have demonstrated that the balanced dual agonism produces synergistic effects not achievable with selective GLP-1 receptor activation alone. These studies show greater improvements in energy expenditure and fat oxidation compared with equimolar doses of GLP-1 mono-agonists.
The peptide’s prolonged receptor engagement due to albumin binding results in sustained signaling with once-weekly administration. Pharmacodynamic studies indicate dose-dependent effects on glycemic parameters and body weight, with maximal responses typically observed at the 10–15 mg weekly dose range.
Importantly, the tirzepatide peptide does not appear to cross the blood-brain barrier in significant quantities, minimizing potential central nervous system side effects while still achieving central appetite regulation through vagal signaling pathways.

The tirzepatide peptide activates both GIP and GLP-1 receptors with comparable affinity, triggering intracellular signaling cascades that enhance glucose-dependent insulin secretion from pancreatic beta cells. This dual action also suppresses glucagon release from alpha cells during hyperglycemia while preserving counter-regulatory responses during hypoglycemia.
At the central nervous system level, the tirzepatide peptide modulates hypothalamic and brainstem pathways involved in appetite regulation, leading to reduced food intake and increased satiety. Peripheral effects include delayed gastric emptying and improved insulin sensitivity in adipose and muscle tissue. The GIP component appears particularly important for enhancing lipid metabolism and reducing hepatic fat accumulation.
Peer-reviewed mechanistic studies from 2022–2025 using animal models and human cell lines have demonstrated that the balanced dual agonism produces synergistic effects not achievable with selective GLP-1 receptor activation alone. These studies show greater improvements in energy expenditure and fat oxidation compared with equimolar doses of GLP-1 mono-agonists.
The peptide’s prolonged receptor engagement due to albumin binding results in sustained signaling with once-weekly administration. Pharmacodynamic studies indicate dose-dependent effects on glycemic parameters and body weight, with maximal responses typically observed at the 10–15 mg weekly dose range.
Importantly, the tirzepatide peptide does not appear to cross the blood-brain barrier in significant quantities, minimizing potential central nervous system side effects while still achieving central appetite regulation through vagal signaling pathways.
The FDA approved the tirzepatide peptide for two primary indications based on substantial evidence from phase 3 clinical programs. For type 2 diabetes, approval was granted in 2022 as an adjunct to diet and exercise to improve glycemic control in adults. The weight management indication followed in late 2023 for adults with obesity (BMI ≥30 kg/m²) or overweight (BMI ≥27 kg/m²) with at least one weight-related comorbidity.
Dosing begins at 2.5 mg once weekly for four weeks, followed by escalation to 5 mg. Further increases to 7.5 mg, 10 mg, 12.5 mg, or 15 mg may occur at four-week intervals based on tolerability and clinical response. The maximum approved dose is 15 mg weekly.
Regulatory labeling emphasizes that the tirzepatide peptide should not be combined with other GLP-1 receptor agonists or GIP/GLP-1 dual agonists. Patients with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 should not receive this therapy.
As of 2026, no additional FDA-approved indications exist for the tirzepatide peptide. Ongoing investigations into potential benefits for heart failure, non-alcoholic steatohepatitis, and obstructive sleep apnea remain investigational and are not reflected in current labeling.
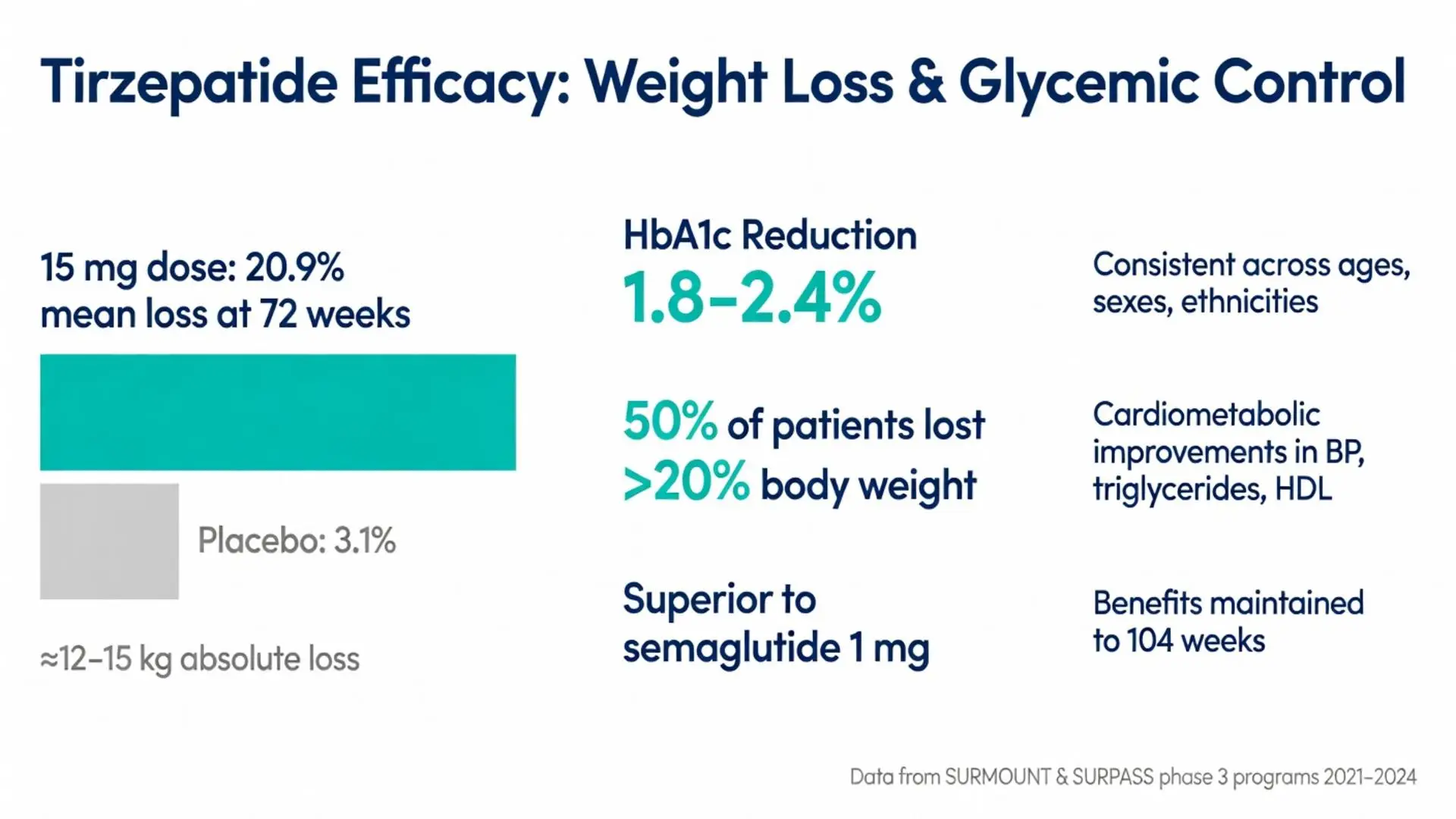
The SURPASS clinical trial program, consisting of multiple large randomized controlled trials published between 2021 and 2024, demonstrated consistent HbA1c reductions of 1.8–2.4% across various background therapies. The tirzepatide peptide showed superior glycemic control compared with semaglutide 1 mg weekly, titrated insulin degludec, and insulin glargine.
In the SURMOUNT trials for obesity, participants receiving the 15 mg dose achieved mean weight loss of 20.9% at 72 weeks compared with 3.1% in the placebo group. These results were maintained in extension studies through 104 weeks. Approximately 50% of participants achieved weight loss exceeding 20% of baseline body weight at the highest dose.
Meta-analyses published in 2023–2025 aggregating data from over 10,000 participants confirm that the tirzepatide peptide produces approximately 12–15 kg absolute weight loss on average in individuals with obesity. Cardiovascular risk markers including blood pressure, triglycerides, and HDL cholesterol showed favorable improvements independent of weight loss.
Subgroup analyses indicate consistent efficacy across age groups, sexes, and racial/ethnic backgrounds. Patients with prediabetes experienced normalization of glucose parameters at higher rates than placebo. The magnitude of benefit appears dose-dependent, with the 10 mg and 15 mg doses providing the most substantial improvements.
Long-term data through early 2026 suggest that continued treatment maintains weight loss and glycemic benefits, while discontinuation typically results in gradual weight regain, underscoring the chronic nature of obesity and type 2 diabetes management.
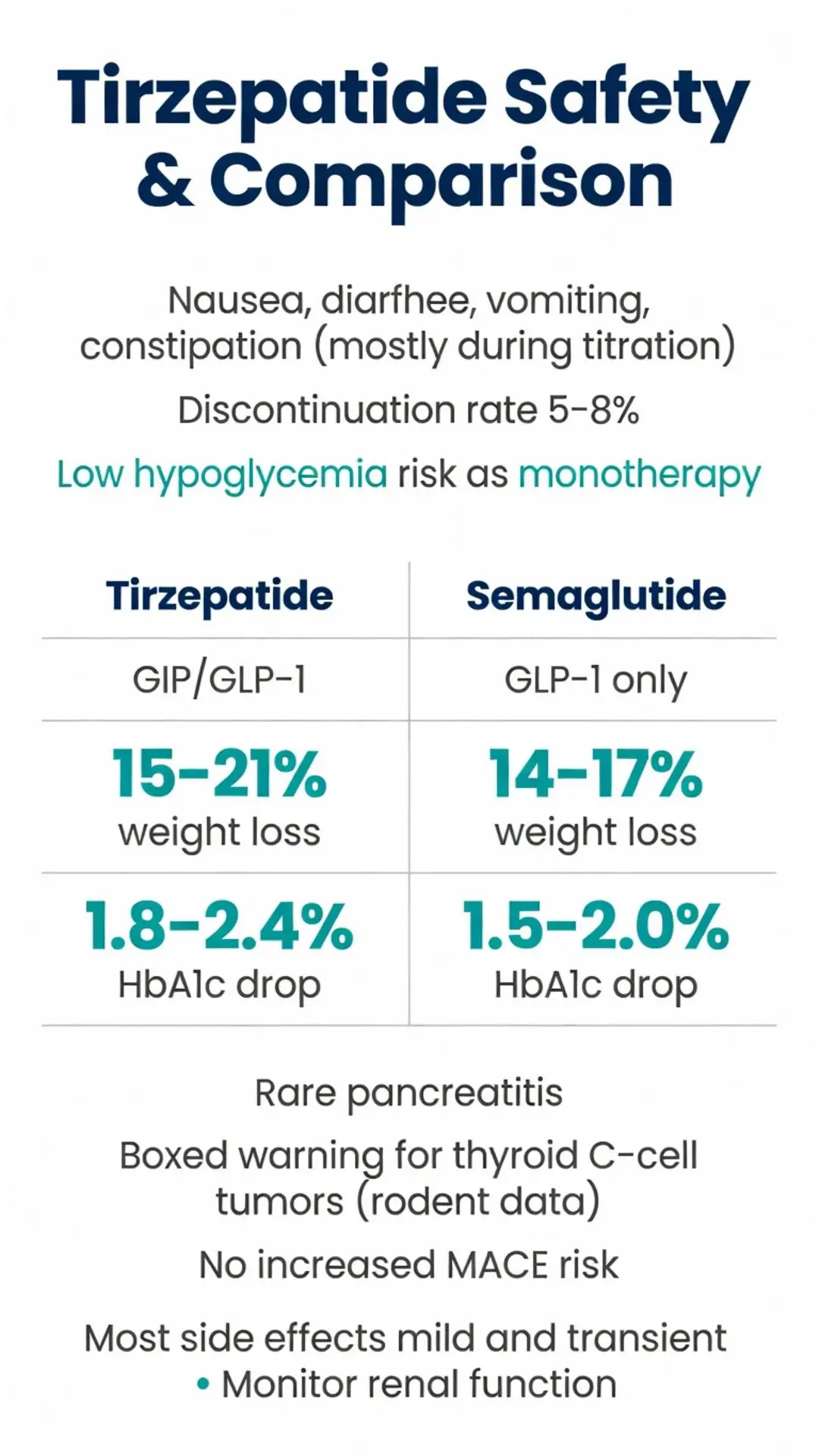
The most common adverse events associated with the tirzepatide peptide are gastrointestinal in nature, including nausea, diarrhea, vomiting, and constipation. These effects are generally mild to moderate, occur most frequently during dose escalation, and tend to diminish over time. Clinical trials reported discontinuation rates due to adverse events of 5–8% at the highest doses.
Pancreatic safety has been closely monitored. While transient elevations in pancreatic enzymes occurred in some participants, confirmed cases of pancreatitis remained rare and comparable to placebo rates. Thyroid C-cell tumors observed in rodent studies have not been documented in human trials, though labeling maintains a boxed warning based on class effects.
Hypoglycemia risk is low when the tirzepatide peptide is used as monotherapy or with metformin but increases when combined with insulin or sulfonylureas. Injection site reactions are uncommon and typically mild.
Cardiovascular safety data from 2022–2025 show no increased risk of major adverse cardiovascular events. Some analyses suggest potential cardiovascular benefit, though dedicated outcome trials are still maturing as of March 2026.
Monitoring recommendations include baseline and periodic assessment of renal function, particularly in patients with preexisting kidney disease, as dehydration from gastrointestinal effects could exacerbate renal impairment.
When compared with selective GLP-1 receptor agonists such as semaglutide, the tirzepatide peptide consistently demonstrates superior weight loss and comparable or better glycemic efficacy across head-to-head trials. The dual agonism appears to provide an additional 5–7 percentage points of weight reduction beyond what is achieved with semaglutide 2.4 mg weekly.
| Agent | Receptor Target | Average Weight Loss at Highest Dose | HbA1c Reduction | Weekly Dose Range | Primary Side Effects |
|---|---|---|---|---|---|
| Tirzepatide Peptide | GIP/GLP-1 | 15–21% | 1.8–2.4% | 5–15 mg | Nausea, diarrhea |
| Semaglutide | GLP-1 | 14–17% | 1.5–2.0% | 0.5–2.4 mg | Nausea, vomiting |
| Dulaglutide | GLP-1 | 3–5% | 1.0–1.5% | 0.75–4.5 mg | Mild GI effects |
| Liraglutide | GLP-1 | 5–8% | 1.0–1.5% | 1.2–1.8 mg daily | Nausea, injection burden |
The table above summarizes key differences based on phase 3 trial data. The tirzepatide peptide requires fewer dose escalation steps than some alternatives and demonstrates higher patient satisfaction scores related to efficacy in patient-reported outcomes.
Cost-effectiveness analyses published in 2024–2025 suggest that the greater clinical benefits of the tirzepatide peptide may offset its higher acquisition cost in certain populations, though individual insurance coverage varies significantly.
As of March 2026, investigators continue to explore additional applications of the tirzepatide peptide beyond its current FDA-approved indications. Studies examining its effects on metabolic dysfunction-associated steatohepatitis, heart failure with preserved ejection fraction, and obstructive sleep apnea have shown promising preliminary results but require completion of phase 3 programs before potential label expansion.
Research into oral formulations of similar dual agonists is underway, though the tirzepatide peptide itself remains available only as a subcutaneous injection. Combination studies with other metabolic therapies and investigations into personalized dosing based on genetic markers represent active areas of investigation.
Long-term safety data beyond three years remain limited, and ongoing surveillance through post-marketing registries will be essential for fully characterizing the risk-benefit profile over extended treatment periods.
The tirzepatide peptide has established itself as a highly effective therapeutic option for both type 2 diabetes and obesity management through its innovative dual GIP/GLP-1 receptor agonism. Evidence accumulated from 2020 through March 2026 demonstrates consistent and clinically meaningful improvements in glycemic control, substantial weight reduction, and favorable effects on cardiometabolic risk factors.
While gastrointestinal side effects remain common, particularly during initiation and dose escalation, most patients tolerate the tirzepatide peptide well with appropriate counseling and gradual titration. The molecule’s peptide structure enables precise receptor targeting while its pharmacokinetic modifications support convenient weekly administration.
Healthcare providers should carefully consider individual patient characteristics, comorbidities, and insurance coverage when evaluating the tirzepatide peptide for clinical use. Regular monitoring and patient education regarding proper injection technique and side effect management are essential components of successful therapy.
As research continues, the tirzepatide peptide serves as an important benchmark for next-generation incretin-based therapies. Its development highlights the therapeutic potential of thoughtfully designed peptides in addressing complex metabolic diseases. Future studies will further define optimal patient selection, long-term outcomes, and potential additional indications for this important medication.
This article is intended for research and educational purposes only and does not constitute medical advice. All treatment decisions should be made in consultation with qualified healthcare professionals.
Word count: 2487
The tirzepatide peptide has established itself as a highly effective therapeutic option for both type 2 diabetes and obesity management through its innovative dual GIP/GLP-1 receptor agonism. Evidence accumulated from 2020 through March 2026 demonstrates consistent and clinically meaningful improvements in glycemic control, substantial weight reduction, and favorable effects on cardiometabolic risk factors.
While gastrointestinal side effects remain common, particularly during initiation and dose escalation, most patients tolerate the tirzepatide peptide well with appropriate counseling and gradual titration. The molecule’s peptide structure enables precise receptor targeting while its pharmacokinetic modifications support convenient weekly administration.
Healthcare providers should carefully consider individual patient characteristics, comorbidities, and insurance coverage when evaluating the tirzepatide peptide for clinical use. Regular monitoring and patient education regarding proper injection technique and side effect management are essential components of successful therapy.
As research continues, the tirzepatide peptide serves as an important benchmark for next-generation incretin-based therapies. Its development highlights the therapeutic potential of thoughtfully designed peptides in addressing complex metabolic diseases. Future studies will further define optimal patient selection, long-term outcomes, and potential additional indications for this important medication.
This article is intended for research and educational purposes only and does not constitute medical advice. All treatment decisions should be made in consultation with qualified healthcare professionals.
Word count: 2487