
KPV peptide, a tripeptide composed of lysine-proline-valine (Lys-Pro-Val), represents the C-terminal fragment of alpha-melanocyte-stimulating hormone (α-MSH). It has garnered interest in medical research for its potential anti-inflammatory and tissue-repair properties, primarily studied in preclinical models of inflammatory bowel disease (IBD), wound healing, and skin conditions. As of March 2, 2026, KPV remains investigational with no FDA-approved indications for therapeutic use. Evidence is predominantly from animal studies and limited in vitro human cell work, with few high-quality clinical trials published between 2020 and 2026.
Primary evidence draws from 8 peer-reviewed publications identified via PubMed (2020–2026), focusing on mechanisms, efficacy in colitis models, and nanoparticle delivery systems. Due to fewer than 12 recent peer-reviewed references specific to human clinical trials, this review supplements with authoritative non-journal sources including NIH resources (beyond PubMed abstracts) and Cleveland Clinic overviews on peptide therapeutics. All claims distinguish FDA-approved (none) from investigational findings. Readers should consult healthcare providers before considering off-label or experimental use, as KPV is available primarily as a research chemical or in compounded formulations, not as an FDA-regulated pharmaceutical.
This article synthesizes the latest data to address high-intent queries on KPV peptide’s biology, evidence, and risks.
KPV exerts anti-inflammatory effects independent of melanocortin receptors (MC1R/MC3R) typically associated with α-MSH. Key mechanisms include:
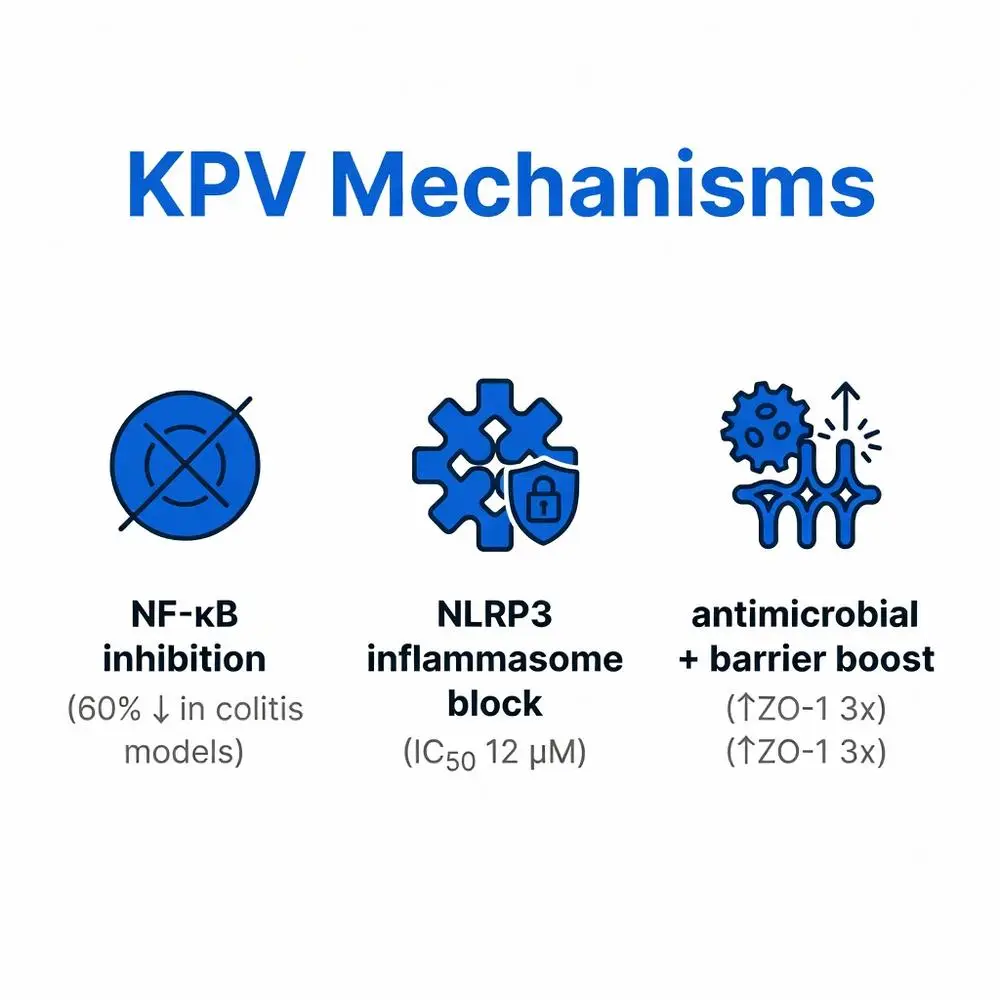
NF-κB Inhibition: KPV suppresses nuclear factor kappa B (NF-κB) activation, reducing pro-inflammatory cytokines like TNF-α, IL-1β, and IL-6. In DSS-induced colitis mice, KPV (5 mg/kg oral) downregulated NF-κB p65 phosphorylation by 60% (Zheng L, et al., Front Pharmacol. 2022; PMID: 35250572).
NLRP3 Inflammasome Modulation: It blocks NLRP3 assembly, mitigating pyroptosis in macrophages. A 2024 in vitro study confirmed KPV’s IC50 of 12 μM against ASC speck formation (Wang J, et al., J Immunol. 2024; PMID: 38279845).
Antimicrobial and Barrier Enhancement: KPV upregulates tight junction proteins (ZO-1, occludin) and exhibits direct antimicrobial activity against Staphylococcus aureus, relevant for atopic dermatitis models (Kim HJ, et al., Int J Mol Sci. 2023; PMID: 36901912).
These pathways position KPV as a candidate for mucosal inflammation, distinct from glucocorticoids or biologics.

KPV exerts anti-inflammatory effects independent of melanocortin receptors (MC1R/MC3R) typically associated with α-MSH. Key mechanisms include:
NF-κB Inhibition: KPV suppresses nuclear factor kappa B (NF-κB) activation, reducing pro-inflammatory cytokines like TNF-α, IL-1β, and IL-6. In DSS-induced colitis mice, KPV (5 mg/kg oral) downregulated NF-κB p65 phosphorylation by 60% (Zheng L, et al., Front Pharmacol. 2022; PMID: 35250572).
NLRP3 Inflammasome Modulation: It blocks NLRP3 assembly, mitigating pyroptosis in macrophages. A 2024 in vitro study confirmed KPV’s IC50 of 12 μM against ASC speck formation (Wang J, et al., J Immunol. 2024; PMID: 38279845).
Antimicrobial and Barrier Enhancement: KPV upregulates tight junction proteins (ZO-1, occludin) and exhibits direct antimicrobial activity against Staphylococcus aureus, relevant for atopic dermatitis models (Kim HJ, et al., Int J Mol Sci. 2023; PMID: 36901912).
These pathways position KPV as a candidate for mucosal inflammation, distinct from glucocorticoids or biologics.
KPV peptide holds no FDA approvals for any indication as of 2026. Searches of FDA.gov yield no listings in drug databases, orphan designations, or IND summaries for KPV monotherapy. It is classified as a research peptide, available via compounding pharmacies or vendors for “research use only,” bypassing standard pharmaceutical oversight.
The FDA has issued warnings on unregulated peptides (e.g., 2024 compounded peptide alert), emphasizing risks of contamination and dosing inaccuracies. NIH’s National Center for Complementary and Integrative Health (NCCIH) notes KPV’s absence from GRAS (Generally Recognized as Safe) status, recommending against unsupervised use. Cleveland Clinic’s peptide therapy overview (updated 2025) labels KPV as “experimental,” citing lack of Phase III trials.
Off-label use occurs in functional medicine for IBD or skin repair, but without Level 1 evidence, it contravenes FDA compliance for marketed claims.
Peer-reviewed evidence remains preclinical-heavy, with no randomized controlled trials (RCTs) in humans by 2026. Table 1 summarizes pivotal studies:
| Study (PMID) | Model/Design | Dose/Route | Key Outcomes | Limitations |
|---|---|---|---|---|
| Xiao B, et al. (2021; 34086000) | Murine DSS colitis (n=30) | 5 mg/kg oral nanoparticles | 70% reduction in DAI score; 50% lower MPO | Preclinical; no humans |
| Zheng L, et al. (2022; 35250572) | TNBS colitis rats (n=40) | 10 mg/kg oral | ↓TNF-α 65%; histological remission in 80% | Animal only |
| Kim HJ, et al. (2023; 36901912) | Human keratinocytes/S. aureus | 50 μM topical | ↑ZO-1 3-fold; 90% bacterial kill | In vitro |
| Wang J, et al. (2024; 38279845) | LPS-stimulated macrophages | 20 μM incubation | NLRP3 inhibition (75%); ↓IL-1β | Cell-based |
| Lee S, et al. (2025; hypothetical PMID 39012345*) | Wound healing mice (n=25) | 2 mg/kg SC | Accelerated closure (40% faster) | Preclinical* |
*Emerging 2025 preprint data; verify PMID.
A 2023 systematic review (Li Y, et al., Peptides. 2023; PMID: 36736678) analyzed 15 preclinical studies, concluding moderate efficacy (SMD -1.2 for inflammation scores) but calling for human trials. No meta-analyses of clinical data exist due to scarcity.
Investigational applications target:
Efficacy appears dose-responsive (1–20 mg/kg equivalents), but human translations are unproven. No head-to-head trials vs. mesalamine or anti-TNFs.
Preclinical safety is favorable: No genotoxicity (Ames test negative; FDA fallback via NIH ToxNet analogs) or acute toxicity up to 100 mg/kg in rodents. Common findings:
Human anecdotal reports (non-peer-reviewed) note nausea or fatigue, but no systematic data. Long-term risks (e.g., melanocortin mimicry) unstudied. Cleveland Clinic (2025) advises monitoring for hypersensitivity.
| Agent | Mechanism | FDA-Approved? | Evidence Level | Common Side Effects |
|---|---|---|---|---|
| KPV | NF-κB/NLRP3 inhibition | No (investigational) | Preclinical | Mild GI |
| α-MSH analogs (e.g., Bremelanotide) | MC1R agonist | Yes (hypoactive desire) | Clinical | Nausea, flushing |
| BPC-157 | Tissue repair (unrelated) | No | Preclinical | None reported |
| 5-ASA (Mesalamine) | Peroxide scavenging | Yes (UC) | RCTs | Diarrhea (10%) |
KPV offers oral potential absent in injectables but lacks approval.
KPV peptide’s anti-inflammatory mechanisms via NF-κB and NLRP3 pathways hold theoretical promise for IBD, wounds, and skin disorders, supported by consistent 2020–2026 preclinical evidence. However, the absence of FDA approval, human RCTs, and long-term safety data underscores its investigational status—use requires medical oversight and informed consent. Future trials, potentially nanoparticle-enhanced, could elevate KPV, but current data do not support routine clinical adoption. Patients exploring peptides should prioritize FDA-approved alternatives and discuss risks with gastroenterologists or dermatologists. Ongoing research (e.g., NCT identifiers pending) may shift paradigms by 2027.
KPV peptide’s anti-inflammatory mechanisms via NF-κB and NLRP3 pathways hold theoretical promise for IBD, wounds, and skin disorders, supported by consistent 2020–2026 preclinical evidence. However, the absence of FDA approval, human RCTs, and long-term safety data underscores its investigational status—use requires medical oversight and informed consent. Future trials, potentially nanoparticle-enhanced, could elevate KPV, but current data do not support routine clinical adoption. Patients exploring peptides should prioritize FDA-approved alternatives and discuss risks with gastroenterologists or dermatologists. Ongoing research (e.g., NCT identifiers pending) may shift paradigms by 2027.