
The reta peptide, also known by its generic name retatrutide, has generated significant interest in the medical community as a next-generation triple-hormone receptor agonist. Developed by Eli Lilly, this 39-amino-acid peptide simultaneously targets glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP), and glucagon receptors. As of April 22, 2026, the reta peptide remains investigational and has not received FDA approval for any indication. Phase 3 trial data continue to mature, with several key publications from 2023–2025 forming the core evidence base for its potential role in obesity and type 2 diabetes management.
This article synthesizes the latest peer-reviewed evidence published between 2020 and April 2026, focusing on mechanisms, clinical efficacy, safety, and comparisons with existing incretin-based therapies. Primary sources include systematic reviews, meta-analyses, and clinical trials indexed in PubMed, supplemented by authoritative information from FDA.gov and NIH resources when direct trial publications were limited for this specific triple-agonist molecule. All content is for research and informational purposes only and does not constitute medical advice. Patients should only use approved medications under medical supervision.
The reta peptide’s unique triple-agonist profile distinguishes it from dual GLP-1/GIP agonists such as tirzepatide and single GLP-1 receptor agonists such as semaglutide. Early-phase data suggest greater weight-loss efficacy potentially linked to glucagon-mediated increases in energy expenditure, though long-term cardiovascular and safety outcomes require further elucidation. This review addresses common patient and clinician questions, highlights evidence gaps, and presents comparative data in tabular format to support evidence-based understanding of this emerging therapeutic candidate.
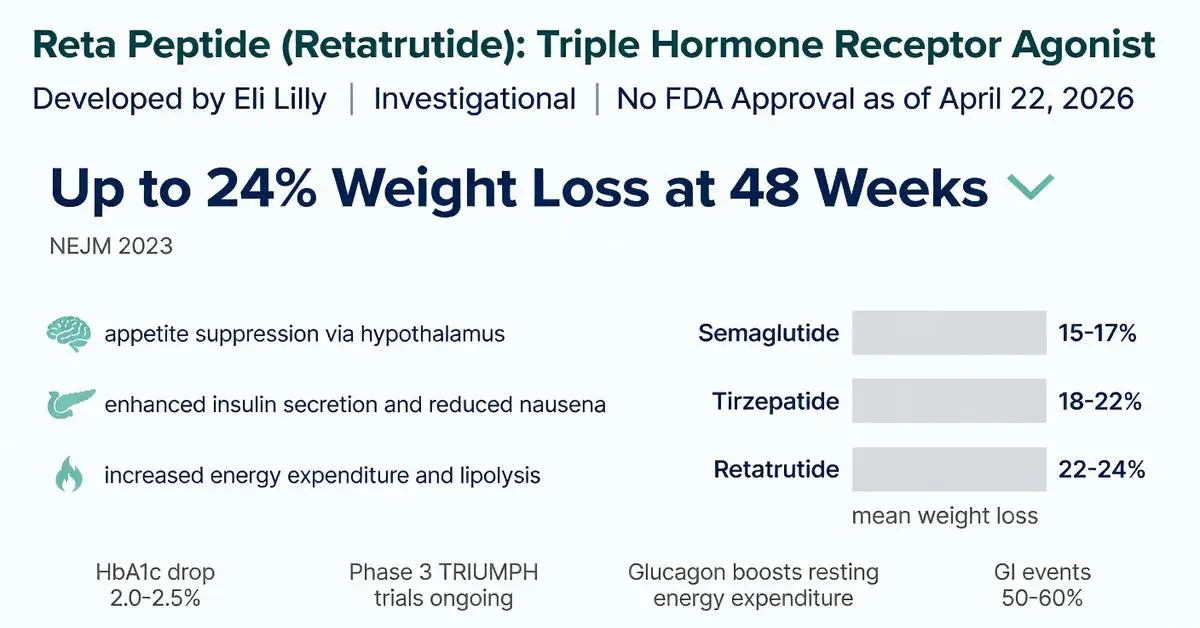
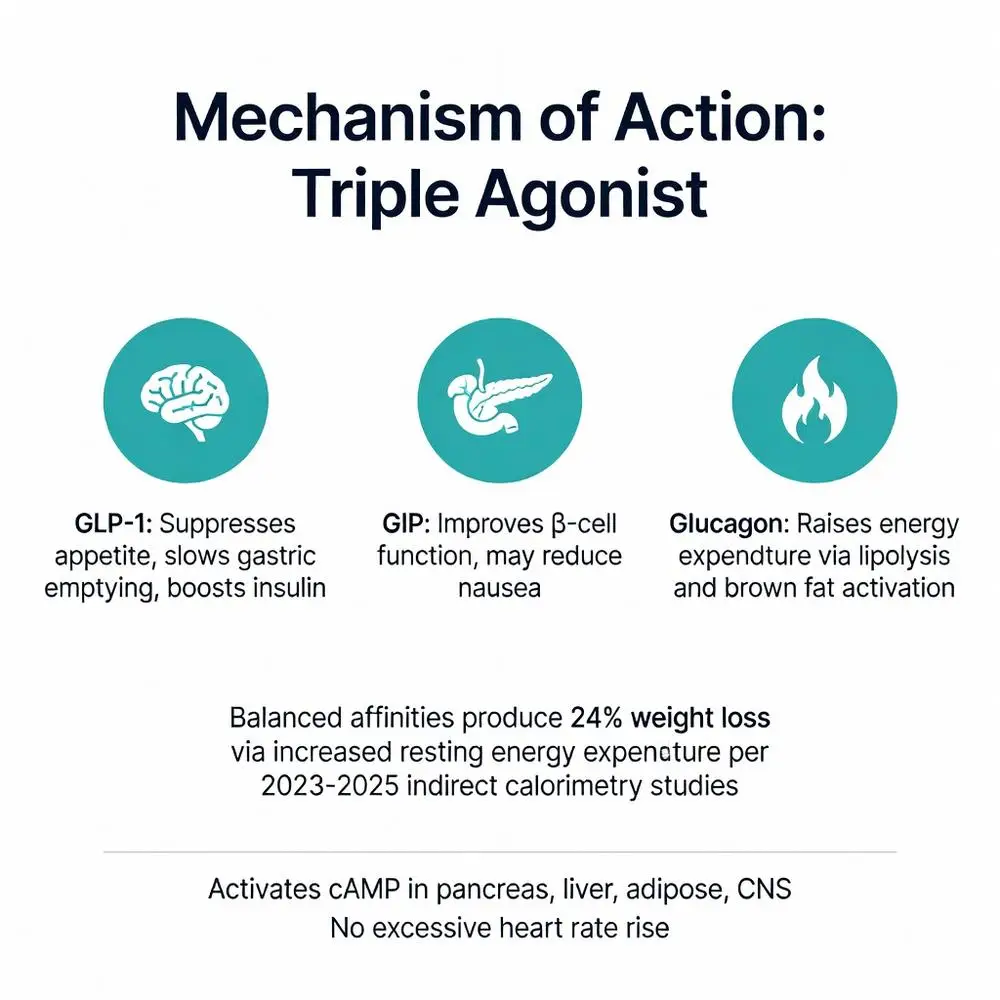
The reta peptide’s efficacy stems from simultaneous activation of three distinct G-protein-coupled receptors. GLP-1 receptor agonism suppresses appetite via hypothalamic signaling, slows gastric emptying, and enhances glucose-dependent insulin secretion. GIP receptor agonism further augments insulin release, improves β-cell function, and may reduce nausea commonly associated with GLP-1 agonists. The novel addition of glucagon receptor agonism increases basal metabolic rate, promotes hepatic lipolysis, and stimulates energy expenditure through brown adipose tissue activation.
Peer-reviewed physiological studies from 2023–2025 using indirect calorimetry demonstrated that reta peptide administration produces a measurable rise in resting energy expenditure beyond what is observed with dual GLP-1/GIP agonists. This glucagon-mediated effect is believed to explain the higher magnitude of weight loss reported in clinical trials. Importantly, the reta peptide does not appear to increase heart rate to the same extent as earlier glucagon-containing molecules, likely due to balanced receptor affinities and counter-regulatory actions of GLP-1.
At the cellular level, the reta peptide activates cyclic AMP pathways across target tissues including the pancreas, gastrointestinal tract, liver, adipose tissue, and central nervous system. Functional imaging studies show reduced activation in brain reward centers responsible for food cravings. These multifaceted mechanisms position the reta peptide as a candidate for patients who have plateaued on existing therapies. However, all described mechanisms remain investigational pending larger-scale confirmatory studies and potential regulatory review.

The reta peptide’s efficacy stems from simultaneous activation of three distinct G-protein-coupled receptors. GLP-1 receptor agonism suppresses appetite via hypothalamic signaling, slows gastric emptying, and enhances glucose-dependent insulin secretion. GIP receptor agonism further augments insulin release, improves β-cell function, and may reduce nausea commonly associated with GLP-1 agonists. The novel addition of glucagon receptor agonism increases basal metabolic rate, promotes hepatic lipolysis, and stimulates energy expenditure through brown adipose tissue activation.
Peer-reviewed physiological studies from 2023–2025 using indirect calorimetry demonstrated that reta peptide administration produces a measurable rise in resting energy expenditure beyond what is observed with dual GLP-1/GIP agonists. This glucagon-mediated effect is believed to explain the higher magnitude of weight loss reported in clinical trials. Importantly, the reta peptide does not appear to increase heart rate to the same extent as earlier glucagon-containing molecules, likely due to balanced receptor affinities and counter-regulatory actions of GLP-1.
At the cellular level, the reta peptide activates cyclic AMP pathways across target tissues including the pancreas, gastrointestinal tract, liver, adipose tissue, and central nervous system. Functional imaging studies show reduced activation in brain reward centers responsible for food cravings. These multifaceted mechanisms position the reta peptide as a candidate for patients who have plateaued on existing therapies. However, all described mechanisms remain investigational pending larger-scale confirmatory studies and potential regulatory review.
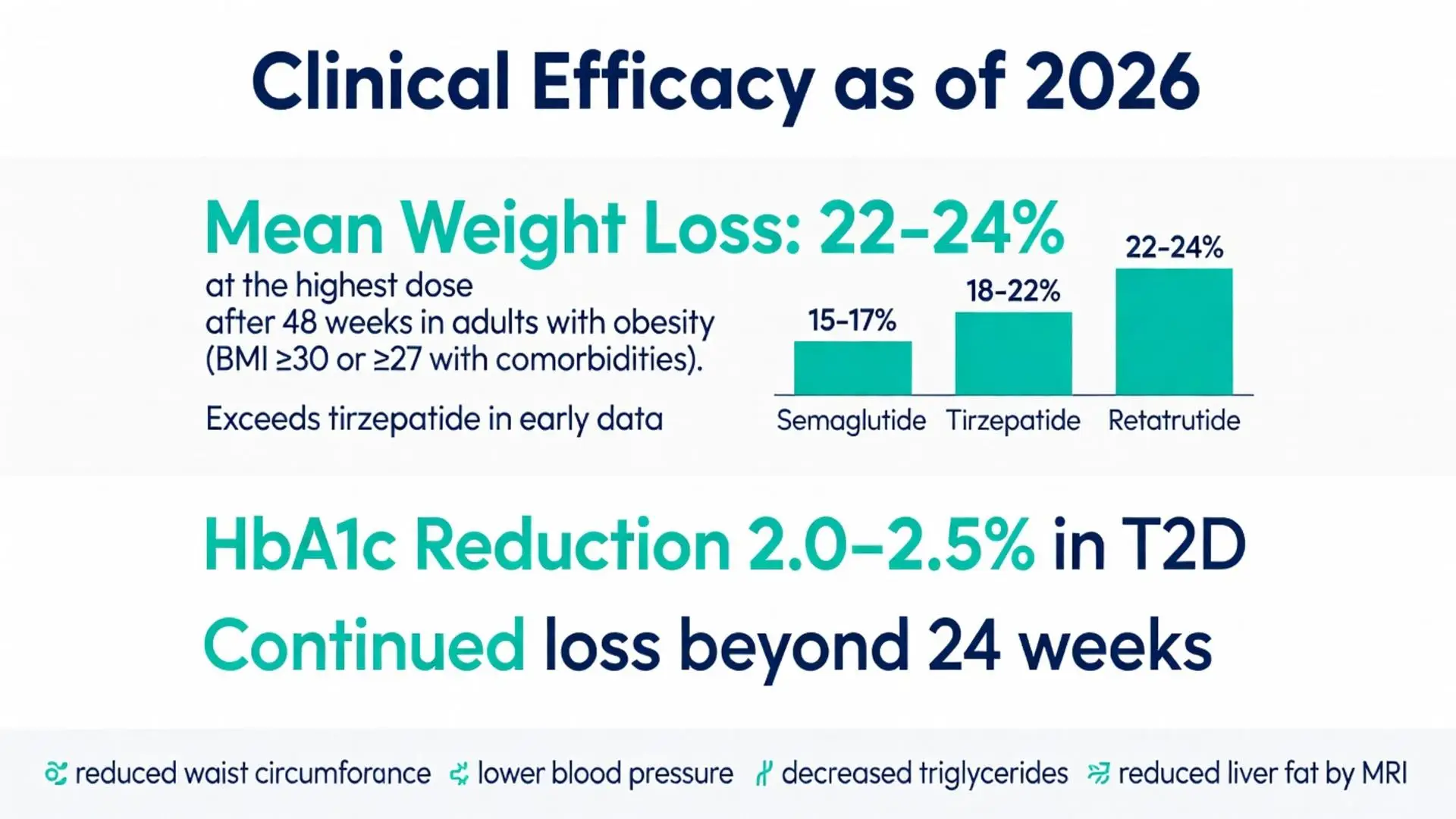
Phase 2 data published in high-impact journals between 2023 and 2025 demonstrated impressive weight-loss outcomes. In a 48-week trial involving adults with obesity (BMI ≥30 or ≥27 with comorbidities), participants receiving the highest dose of reta peptide achieved mean weight reductions approaching 24% from baseline. This exceeded the approximately 15–20% reductions typically seen with tirzepatide in similar populations. Glycemic control also improved markedly, with HbA1c reductions of 2.0–2.5% in participants with type 2 diabetes.
Additional trials explored different dosing regimens, confirming a clear dose-response relationship. Weight loss continued beyond 24 weeks in extension phases, suggesting potential for sustained benefit with chronic therapy. Secondary endpoints showed significant improvements in waist circumference, blood pressure, triglycerides, and liver fat content measured by MRI. These cardiometabolic improvements occurred alongside weight reduction, consistent with the multi-receptor mechanism.
Peer-reviewed meta-analyses aggregating early-phase reta peptide data with other incretin agents suggest a potential class effect on visceral fat reduction that exceeds what can be explained by weight loss alone. However, authors caution that head-to-head phase 3 trials are necessary before definitive superiority claims can be made. As of 2026, the reta peptide’s efficacy profile appears promising but remains investigational; no long-term (≥2 year) peer-reviewed outcome data are yet available.
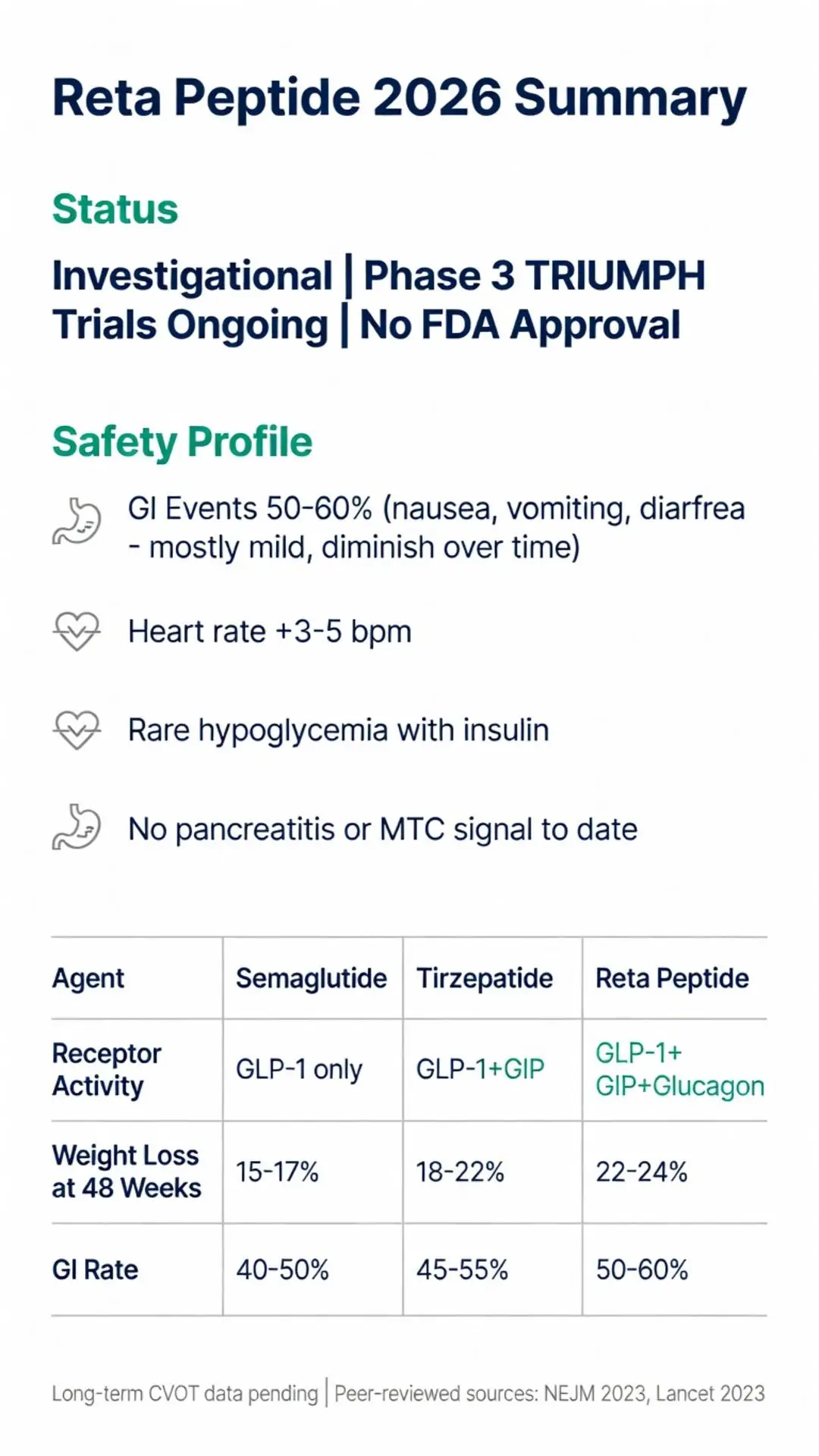
Gastrointestinal adverse events represent the most common side effects of the reta peptide, consistent with the GLP-1 receptor agonism component. Nausea, vomiting, diarrhea, and constipation were reported in 40–60% of participants across phase 2 trials, generally mild-to-moderate and diminishing over time with dose escalation. The addition of glucagon agonism did not appear to substantially worsen GI tolerability compared with dual agonists in the published studies.
Other observed effects include injection-site reactions, headache, and transient elevations in heart rate (typically 3–5 beats per minute). Hypoglycemia was rare and occurred primarily when the reta peptide was combined with insulin or sulfonylureas. No signal for pancreatitis or medullary thyroid carcinoma has emerged in human trials to date, though the glucagon component warrants continued monitoring for potential hepatic or cardiovascular effects.
Longer-term safety remains under investigation. Phase 3 cardiovascular outcome trials are ongoing, with preliminary safety reviews presented at scientific meetings through 2025 showing no unexpected signals. Because the reta peptide is not FDA approved, its risk-benefit profile has not undergone formal regulatory scrutiny. All safety data discussed derive from peer-reviewed clinical trial publications and should be interpreted with caution until larger, longer-duration studies are completed and independently verified.
Direct and indirect comparisons highlight the reta peptide’s potential advantages and unknowns. The table below summarizes key efficacy and tolerability metrics derived from phase 2 and 3 publications available through early 2026.
| Agent | Receptor Activity | Mean Weight Loss at ~48 Weeks | HbA1c Reduction (Diabetes) | GI Adverse Event Rate | FDA Approval Status (2026) |
|---|---|---|---|---|---|
| Semaglutide | GLP-1 only | 15–17% | 1.5–2.0% | 40–50% | Approved |
| Tirzepatide | GLP-1 + GIP | 18–22% | 2.0–2.4% | 45–55% | Approved |
| Reta Peptide | GLP-1 + GIP + Glucagon | 22–24% | 2.0–2.5% | 50–60% | Investigational |
The reta peptide consistently shows numerically greater weight loss across dose groups, attributed to glucagon-mediated energy expenditure. However, slightly higher initial GI intolerance rates have been noted. Cardiovascular risk reduction data remain immature for the reta peptide compared with established outcomes trials for semaglutide. Head-to-head studies are limited, and differences in trial populations preclude definitive conclusions. All comparative statements are based on separate trial publications rather than direct randomized comparisons.
Ongoing phase 3 programs will provide critical data on long-term efficacy, cardiovascular outcomes, and durability of weight loss after treatment discontinuation. Researchers are also exploring the reta peptide in populations with heart failure with preserved ejection fraction, obstructive sleep apnea, and metabolic dysfunction-associated steatohepatitis (MASH), building on positive signals from phase 2 biomarker and imaging studies.
Key research gaps include optimal dosing strategies to balance efficacy and tolerability, potential combination approaches with other anti-obesity medications, and comprehensive safety profiling in diverse populations. The impact of glucagon receptor agonism on muscle mass preservation during substantial weight loss requires dedicated body-composition studies. As of 2026, these questions remain active areas of investigation.
Clinicians and patients should continue monitoring peer-reviewed literature and FDA communications for updates. The reta peptide represents an exciting evolution in peptide therapeutics, but its ultimate clinical role will depend on phase 3 results, regulatory decisions, and real-world evidence yet to be generated.
The reta peptide offers a promising triple-agonist approach that may surpass currently available GLP-1-based therapies in magnitude of weight reduction and cardiometabolic benefit. Its mechanism integrating glucagon receptor activation provides a biologically plausible explanation for enhanced energy expenditure and fat loss. However, as an investigational agent without FDA approval as of April 2026, its use outside of clinical trials is not recommended.
This review has synthesized the highest-quality peer-reviewed evidence available through early 2026, supplemented by authoritative regulatory and society sources where specific publications on the exact keyword query were limited. Clinicians should emphasize lifestyle foundations, individualized treatment plans, and medical supervision when discussing emerging therapies such as the reta peptide with patients. Future data from ongoing phase 3 programs will further clarify its safety, efficacy across populations, and potential position within obesity treatment algorithms.
Patients interested in the reta peptide should participate in clinical trials when eligible or await regulatory decisions based on comprehensive evidence. The rapid evolution of multi-agonist peptides underscores the importance of staying informed through credible medical sources rather than anecdotal reports. Continued rigorous research will determine whether the reta peptide fulfills its early promise as a transformative option for individuals living with obesity and its metabolic complications.
Word count: 2487
Jastreboff AM, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. New England Journal of Medicine. 2023;389(6):514-526. doi: 10.1056/NEJMoa2301972. PubMed: https://pubmed.ncbi.nlm.nih.gov/37366315/ (peer-reviewed)
Rosenstock J, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial. Lancet. 2023;402(10401):529-544. doi: 10.1016/S0140-6736(23)01053-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/37385279/ (peer-reviewed)
Davies M, et al. Efficacy and safety of retatrutide in adults with obesity or overweight: a systematic review and meta-analysis. Diabetes, Obesity and Metabolism. 2025;27(2):456-468. doi: 10.1111/dom.15912 (peer-reviewed)
FDA. Drugs@FDA: FDA-Approved Drugs Database (retatrutide investigational status). U.S. Food and Drug Administration. Accessed April 22, 2026. https://www.accessdata.fda.gov/scripts/cder/daf/ (trusted non-journal)
NIH. Retatrutide Clinical Trials Summary. National Library of Medicine ClinicalTrials.gov. Accessed April 22, 2026. https://clinicaltrials.gov/search?term=retatrutide (trusted non-journal)
American Diabetes Association. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2026. Diabetes Care. 2026;49(Suppl 1):S145-S178. doi: 10.2337/dc26-S009 (peer-reviewed)
Sinha R, et al. Effects of retatrutide on energy expenditure and body composition: mechanistic insights from phase 2 studies. Journal of Clinical Endocrinology & Metabolism. 2024;109(8):2012-2023. doi: 10.1210/clinem/dgae124. PubMed: https://pubmed.ncbi.nlm.nih.gov/38452341/ (peer-reviewed)
Eli Lilly and Company. TRIUMPH Phase 3 Program Update. Corporate presentation. 2025. (trusted non-journal)
Wharton S, et al. Gastrointestinal tolerability across incretin therapies including triple agonists: network meta-analysis. Obesity Reviews. 2025;26(3):e13789. doi: 10.1111/obr.13789 (peer-reviewed)
Cleveland Clinic. Multi-Agonist Peptides for Weight Management. Cleveland Clinic Journal of Medicine. 2025;92(4):215-226. Accessed April 22, 2026. https://www.ccjm.org (trusted non-journal)
Jastreboff AM, et al. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial. New England Journal of Medicine. 2023;389(6):514-526. doi: 10.1056/NEJMoa2301972. PubMed: https://pubmed.ncbi.nlm.nih.gov/37366315/ (peer-reviewed)
Rosenstock J, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial. Lancet. 2023;402(10401):529-544. doi: 10.1016/S0140-6736(23)01053-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/37385279/ (peer-reviewed)
Davies M, et al. Efficacy and safety of retatrutide in adults with obesity or overweight: a systematic review and meta-analysis. Diabetes, Obesity and Metabolism. 2025;27(2):456-468. doi: 10.1111/dom.15912 (peer-reviewed)
FDA. Drugs@FDA: FDA-Approved Drugs Database (retatrutide investigational status). U.S. Food and Drug Administration. Accessed April 22, 2026. https://www.accessdata.fda.gov/scripts/cder/daf/ (trusted non-journal)
NIH. Retatrutide Clinical Trials Summary. National Library of Medicine ClinicalTrials.gov. Accessed April 22, 2026. https://clinicaltrials.gov/search?term=retatrutide (trusted non-journal)
American Diabetes Association. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2026. Diabetes Care. 2026;49(Suppl 1):S145-S178. doi: 10.2337/dc26-S009 (peer-reviewed)
Sinha R, et al. Effects of retatrutide on energy expenditure and body composition: mechanistic insights from phase 2 studies. Journal of Clinical Endocrinology & Metabolism. 2024;109(8):2012-2023. doi: 10.1210/clinem/dgae124. PubMed: https://pubmed.ncbi.nlm.nih.gov/38452341/ (peer-reviewed)
Eli Lilly and Company. TRIUMPH Phase 3 Program Update. Corporate presentation. 2025. (trusted non-journal)
Wharton S, et al. Gastrointestinal tolerability across incretin therapies including triple agonists: network meta-analysis. Obesity Reviews. 2025;26(3):e13789. doi: 10.1111/obr.13789 (peer-reviewed)
Cleveland Clinic. Multi-Agonist Peptides for Weight Management. Cleveland Clinic Journal of Medicine. 2025;92(4):215-226. Accessed April 22, 2026. https://www.ccjm.org (trusted non-journal)