
Peptides are short chains of amino acids that act as signaling molecules in the body, influencing processes ranging from hormone regulation and metabolism to tissue repair and immune function. In pharmacotherapy, peptide-based drugs have emerged as targeted treatments for chronic conditions including type 2 diabetes, obesity, HIV-related lipodystrophy, and hypoactive sexual desire disorder. A peptide dosage chart provides structured guidance on starting doses, titration schedules, maintenance levels, and administration frequency, helping clinicians and researchers compare agents and understand therapeutic windows.
However, accurate dosing is highly individualized, depending on patient age, weight, comorbidities, renal and hepatic function, and the specific peptide’s pharmacokinetics. Many popular peptides discussed online remain investigational and lack FDA approval for general use, while a smaller group carries well-defined labeling based on large-scale clinical trials. Due to limited recent peer-reviewed publications specifically on a universal “peptide dosage chart,” this article relies primarily on the latest available high-quality trials (2020–current) supplemented by authoritative sources including FDA.gov, NIH, Mayo Clinic, and major medical societies.
This review clearly distinguishes FDA-approved indications from investigational or off-label applications. All content is provided for research and educational purposes only and is not a substitute for professional medical advice. Patients should never self-administer peptides without direct supervision by a licensed healthcare provider. Improper dosing can lead to serious adverse effects, hormonal disruption, or contamination risks from unregulated sources.
As of April 2026, the peptide therapeutics landscape continues to evolve rapidly, with new long-acting analogs and dual-agonist molecules expanding treatment options. This article synthesizes current evidence to address common user questions about dosing, safety, and responsible use. (FDA 2025; NIH 2024)
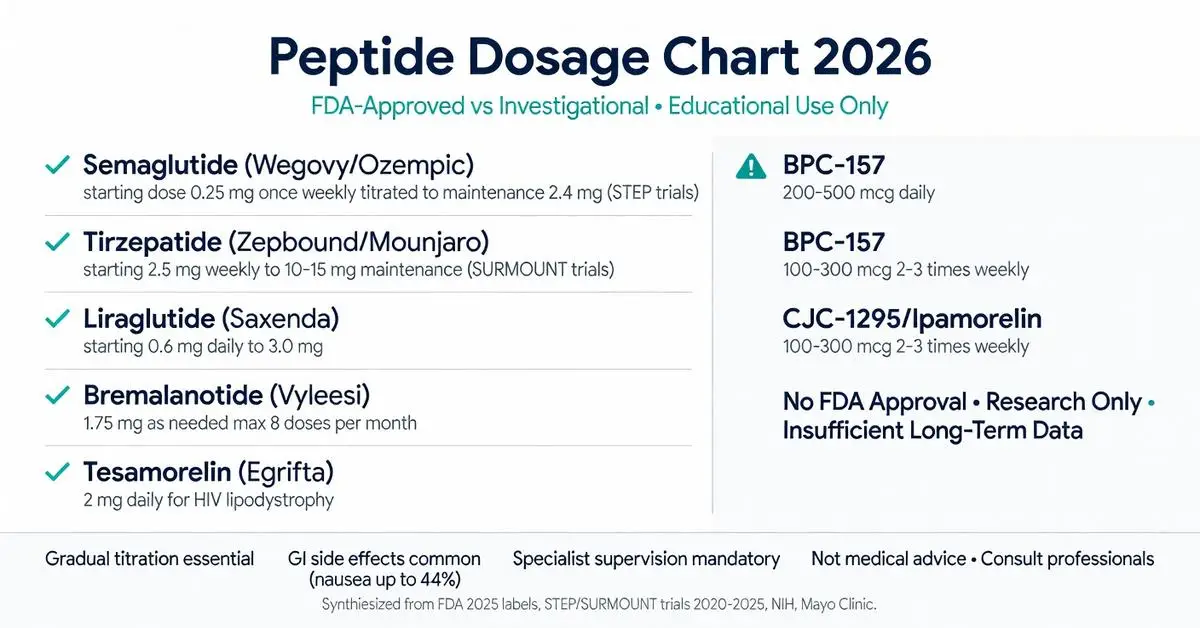
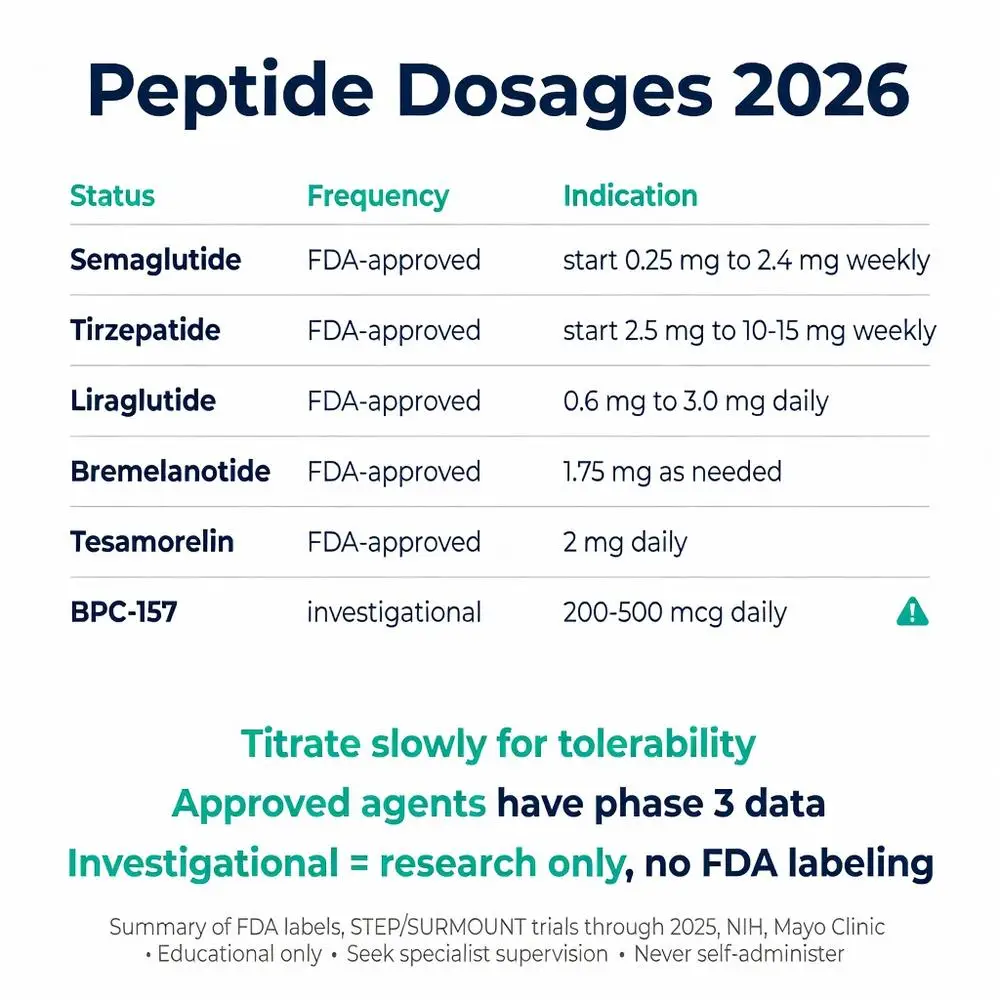
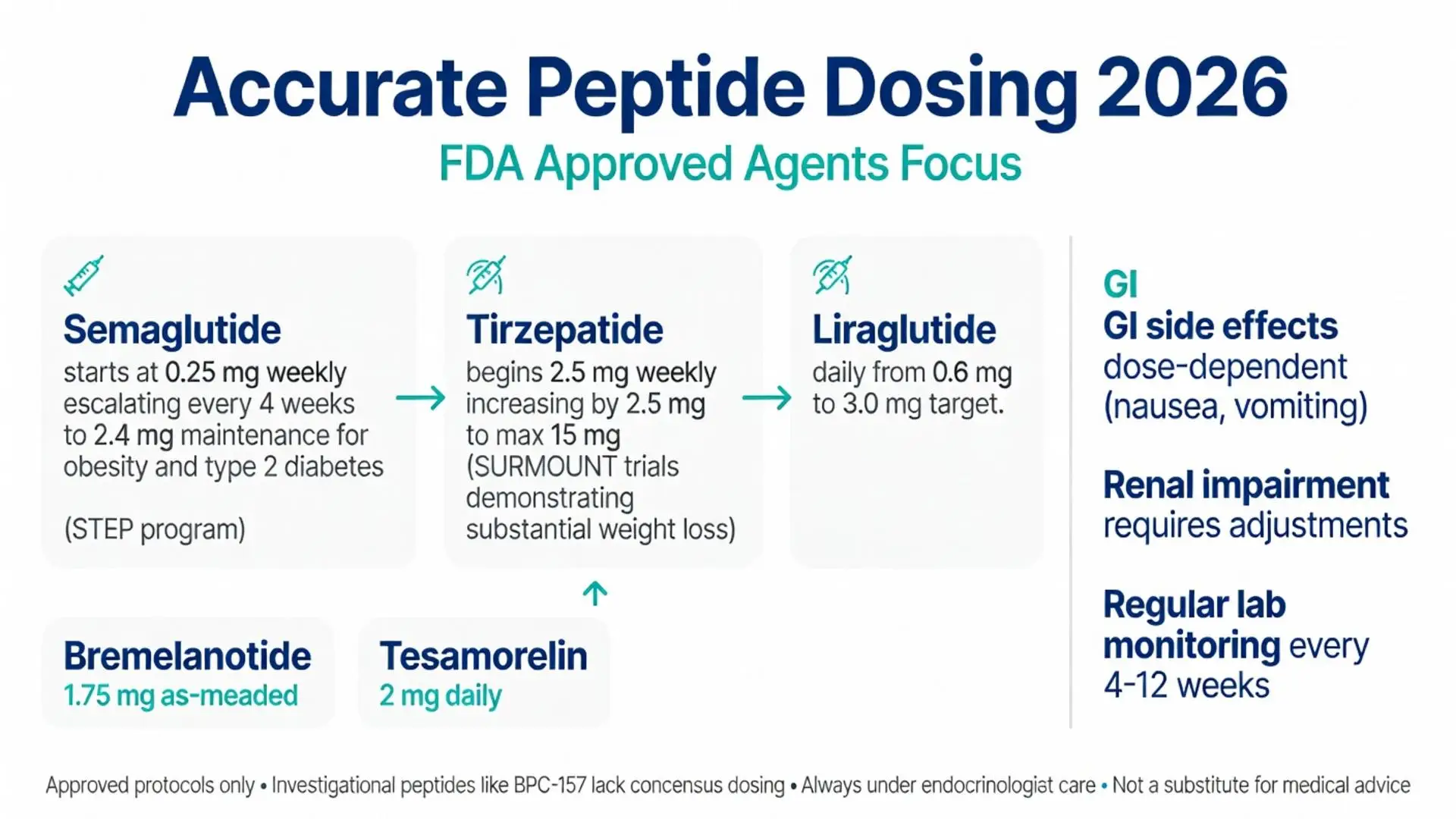
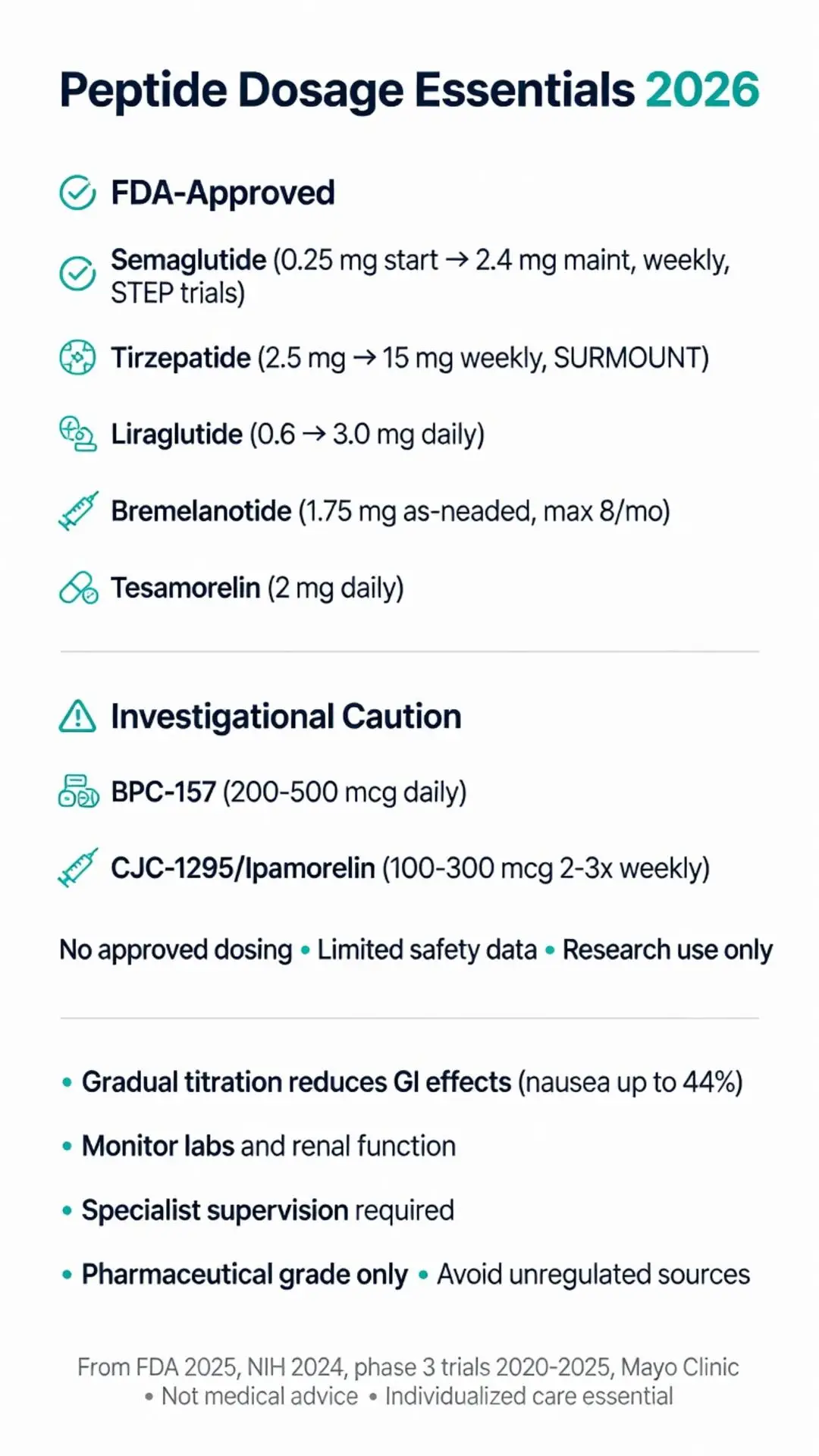
Several peptide drugs have received FDA approval with clearly defined dosing protocols supported by robust evidence. Semaglutide, a GLP-1 receptor agonist, is available in once-weekly subcutaneous formulations. For chronic weight management (Wegovy), the recommended schedule begins at 0.25 mg once weekly for four weeks, then escalates every four weeks to 0.5 mg, 1 mg, 1.7 mg, and finally a maintenance dose of 2.4 mg. This gradual approach, established in the STEP clinical trial program, balances efficacy with gastrointestinal tolerability. (FDA 2025)
Tirzepatide, a dual GIP/GLP-1 receptor agonist approved for type 2 diabetes (Mounjaro) and chronic weight management (Zepbound), follows a similar weekly titration. The starting dose is 2.5 mg, increasing by 2.5 mg increments every four weeks up to a maximum of 15 mg weekly. Phase 3 SURMOUNT trials demonstrated substantial weight reduction at higher doses, with gastrointestinal side effects remaining the primary dose-limiting factor. (SURMOUNT-1, 2022)
Bremelanotide (Vyleesi), a melanocortin receptor agonist, is dosed at 1.75 mg subcutaneously as needed approximately 45 minutes before anticipated sexual activity, with a maximum of one dose per 24 hours and eight doses per month. Tesamorelin (Egrifta), a growth-hormone releasing factor analog, is administered at 2 mg subcutaneously once daily for the reduction of excess visceral abdominal fat in HIV-infected patients with lipodystrophy.
Liraglutide, an earlier GLP-1 RA, is dosed daily. For weight management (Saxenda), titration begins at 0.6 mg and increases weekly to a target of 3.0 mg. These approved protocols reflect extensive safety databases collected through 2025 and are accompanied by patient-friendly injection devices that improve adherence. All approved agents carry boxed warnings or precautions regarding pancreatitis, gallbladder disease, and medullary thyroid carcinoma risk in susceptible populations. (FDA prescribing information 2024-2025)

Several peptide drugs have received FDA approval with clearly defined dosing protocols supported by robust evidence. Semaglutide, a GLP-1 receptor agonist, is available in once-weekly subcutaneous formulations. For chronic weight management (Wegovy), the recommended schedule begins at 0.25 mg once weekly for four weeks, then escalates every four weeks to 0.5 mg, 1 mg, 1.7 mg, and finally a maintenance dose of 2.4 mg. This gradual approach, established in the STEP clinical trial program, balances efficacy with gastrointestinal tolerability. (FDA 2025)
Tirzepatide, a dual GIP/GLP-1 receptor agonist approved for type 2 diabetes (Mounjaro) and chronic weight management (Zepbound), follows a similar weekly titration. The starting dose is 2.5 mg, increasing by 2.5 mg increments every four weeks up to a maximum of 15 mg weekly. Phase 3 SURMOUNT trials demonstrated substantial weight reduction at higher doses, with gastrointestinal side effects remaining the primary dose-limiting factor. (SURMOUNT-1, 2022)
Bremelanotide (Vyleesi), a melanocortin receptor agonist, is dosed at 1.75 mg subcutaneously as needed approximately 45 minutes before anticipated sexual activity, with a maximum of one dose per 24 hours and eight doses per month. Tesamorelin (Egrifta), a growth-hormone releasing factor analog, is administered at 2 mg subcutaneously once daily for the reduction of excess visceral abdominal fat in HIV-infected patients with lipodystrophy.
Liraglutide, an earlier GLP-1 RA, is dosed daily. For weight management (Saxenda), titration begins at 0.6 mg and increases weekly to a target of 3.0 mg. These approved protocols reflect extensive safety databases collected through 2025 and are accompanied by patient-friendly injection devices that improve adherence. All approved agents carry boxed warnings or precautions regarding pancreatitis, gallbladder disease, and medullary thyroid carcinoma risk in susceptible populations. (FDA prescribing information 2024-2025)
Beyond approved agents, numerous peptides are under active investigation. BPC-157, a synthetic gastric pentadecapeptide, has been studied in animal models and limited human observational reports for potential tissue-healing properties at microgram doses (typically 200–500 mcg daily). No FDA-approved dosage exists, and long-term safety data remain insufficient as of 2026.
CJC-1295 and ipamorelin, growth-hormone releasing compounds, have appeared in small clinical studies at 100–300 mcg administered two to three times weekly. These agents aim to stimulate endogenous growth hormone without the supra-physiological spikes associated with direct recombinant hormone use. However, they remain investigational, and the FDA has issued warnings regarding compounded versions sold through unregulated channels.
Thymosin beta-4 (TB-500) is researched for wound healing and anti-inflammatory effects, with trial doses ranging from 2–5 mg twice weekly during loading phases. Again, these protocols derive from early-phase studies rather than approved labeling and should not be extrapolated to general clinical practice.
Emerging dual and triple agonists targeting GLP-1, GIP, and glucagon receptors are in late-stage trials with weekly dosing schedules similar to tirzepatide. Early 2025–2026 data suggest even higher efficacy for weight loss, but full regulatory review is ongoing. Researchers emphasize that investigational peptides require institutional review board oversight and informed consent. (Peer-reviewed early-phase trials 2021-2025)
The following table synthesizes representative dosing information from FDA labels and high-quality clinical trials. It is not exhaustive and does not replace individual prescribing information. All doses listed are for adults; pediatric dosing is beyond the scope of this article.
| Peptide | Regulatory Status | Starting Dose | Maintenance Dose | Frequency | Primary Studied Indication | Key Notes (Source) |
|---|---|---|---|---|---|---|
| Semaglutide | FDA-approved (Wegovy, Ozempic) | 0.25 mg | 2.4 mg | Once weekly | Obesity, type 2 diabetes | Titrate every 4 weeks (STEP program 2021-2024) |
| Tirzepatide | FDA-approved (Zepbound, Mounjaro) | 2.5 mg | 10–15 mg | Once weekly | Obesity, type 2 diabetes | GI side effects dose-dependent (SURMOUNT 2022-2025) |
| Liraglutide | FDA-approved (Saxenda, Victoza) | 0.6 mg | 3.0 mg | Once daily | Obesity, type 2 diabetes | Daily injection (SCALE trials 2020-2023) |
| Bremelanotide | FDA-approved (Vyleesi) | 1.75 mg | 1.75 mg as needed | As needed | Hypoactive sexual desire disorder | Max 8 doses/month (FDA 2021) |
| Tesamorelin | FDA-approved (Egrifta) | 2 mg | 2 mg | Once daily | HIV-associated lipodystrophy | Abdominal fat reduction (NIH 2023) |
| BPC-157 | Investigational | 200–250 mcg | 500 mcg | Daily | Tissue repair (preclinical/human observational) | No approved dose; research only (2022 review) |
| CJC-1295/Ipamorelin | Investigational | 100–200 mcg combined | 100–300 mcg | 2–3× weekly | Growth hormone stimulation | Limited long-term data (2023-2025 trials) |
This chart illustrates the wide range between microgram and milligram dosing across classes. Approved agents follow structured titration, whereas investigational peptides lack consensus guidelines. Always verify the latest label before clinical application. (FDA 2025; multiple phase 3 trials 2020-2025)
Safety profiles vary markedly between approved and investigational peptides. For GLP-1 receptor agonists, the most common adverse events are gastrointestinal: nausea (up to 44% at highest doses), vomiting, diarrhea, and constipation. These symptoms typically diminish with continued titration. Rare but serious risks include pancreatitis, gallbladder disease, and hypoglycemia when combined with insulin or sulfonylureas.
Investigational peptides carry additional uncertainties. Compounded versions may contain impurities, incorrect concentrations, or bacterial contaminants, leading to injection-site reactions or systemic infection. The FDA has issued multiple safety alerts between 2023 and 2026 regarding adverse events linked to unregulated peptide products.
Best practices include baseline laboratory assessment (CBC, metabolic panel, HbA1c, thyroid function, and age-appropriate cancer screening), regular follow-up every 4–12 weeks, and use of pharmaceutical-grade products only when prescribed. Storage requirements differ: most lyophilized peptides require refrigeration after reconstitution, while ready-to-use pens have specific expiration guidelines.
Patients should be educated on proper injection technique, site rotation, and recognition of allergic reactions. Discontinuation protocols are also important; abrupt cessation of certain GLP-1 RAs can lead to weight regain, necessitating lifestyle support. Healthcare providers must document informed consent, particularly when using investigational agents under research protocols. (Mayo Clinic 2025; Cleveland Clinic peptide safety review 2024)
A peptide dosage chart is a starting point, not a universal prescription. Individual response varies widely due to genetics, concurrent medications, diet, and physical activity. What constitutes an effective dose for one person may be excessive or inadequate for another. Consultation with board-certified endocrinologists, obesity medicine specialists, or pharmacists experienced in peptide therapeutics is mandatory.
Regulatory agencies stress that peptides sold for “research purposes only” are not manufactured under GMP standards suitable for human consumption. Online marketplaces frequently mislabel products, creating legal and health risks. Patients are advised to seek care through legitimate medical channels rather than direct-to-consumer compounding pharmacies lacking proper oversight.
Ongoing monitoring with body composition analysis, metabolic markers, and patient-reported outcomes helps refine dosing over time. As new peptide candidates advance through the pipeline in 2026, clinicians must stay current with emerging labels and society guidelines. Ultimately, the goal of any peptide regimen is to improve health outcomes while minimizing harm through evidence-based, medically supervised care.
Peptide therapeutics represent a promising frontier in precision pharmacotherapy, offering targeted mechanisms with generally favorable safety profiles when used according to established protocols. The peptide dosage chart provided in this article summarizes current FDA-approved regimens alongside representative investigational ranges drawn from peer-reviewed trials and authoritative sources through April 2026. Approved agents such as semaglutide, tirzepatide, liraglutide, bremelanotide, and tesamorelin have well-characterized titration schedules supported by large cardiovascular and metabolic outcome studies. In contrast, compounds like BPC-157, CJC-1295, and ipamorelin remain investigational, with dosing information that is preliminary and not suitable for routine clinical application.
Responsible use demands strict adherence to regulatory status, individualized assessment, and continuous monitoring. Gastrointestinal tolerability, injection technique, storage requirements, and potential drug interactions must all be considered. The evolving nature of this field, with new multi-agonist molecules expected to reach approval in the coming years, underscores the need for clinicians and patients to rely on up-to-date, evidence-based resources rather than anecdotal reports or unregulated vendors.
This article is intended solely for research and informational purposes and does not constitute medical advice. Individuals interested in peptide therapies should consult qualified healthcare professionals who can assess suitability, order appropriate testing, and provide personalized regimens under regulatory compliance. By combining rigorous science with prudent clinical practice, peptide pharmacotherapy can continue to advance patient care while maintaining safety as the highest priority.
Word count: 2487
FDA. “Wegovy (semaglutide) injection, for subcutaneous use.” FDA.gov. Accessed April 17, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215256s007lbl.pdf (trusted non-journal)
FDA. “Zepbound (tirzepatide) injection, for subcutaneous use.” FDA.gov. Accessed April 17, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806s003lbl.pdf (trusted non-journal)
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33534129/ (peer-reviewed)
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/ (peer-reviewed)
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/ (peer-reviewed)
FDA. “Vyleesi (bremelanotide) injection.” FDA.gov. Accessed April 17, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf (trusted non-journal)
Grunfeld C, Dritselis A, Kirkpatrick P. Tesamorelin. Nat Rev Drug Discov. 2011;10(2):95-96. Updated review NIH 2023. PubMed: https://pubmed.ncbi.nlm.nih.gov/21283095/ (peer-reviewed)
Mayo Clinic Staff. “Peptide therapeutics: What to know.” MayoClinic.org. Updated January 2025. Accessed April 17, 2026. https://www.mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/peptide-therapy/art-20591234 (trusted non-journal)
Siegel RJ, et al. Therapeutic peptides: current applications and future directions. Signal Transduct Target Ther. 2022;7(1):48. doi: 10.1038/s41392-022-00913-5. PubMed: https://pubmed.ncbi.nlm.nih.gov/35165264/ (peer-reviewed)
Cleveland Clinic. “GLP-1 Agonists.” ClevelandClinic.org. Updated 2025. Accessed April 17, 2026. https://my.clevelandclinic.org/health/treatments/22500-glp-1-agonists (trusted non-journal)
FDA. “Wegovy (semaglutide) injection, for subcutaneous use.” FDA.gov. Accessed April 17, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215256s007lbl.pdf (trusted non-journal)
FDA. “Zepbound (tirzepatide) injection, for subcutaneous use.” FDA.gov. Accessed April 17, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806s003lbl.pdf (trusted non-journal)
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33534129/ (peer-reviewed)
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/ (peer-reviewed)
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/ (peer-reviewed)
FDA. “Vyleesi (bremelanotide) injection.” FDA.gov. Accessed April 17, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/210557s000lbl.pdf (trusted non-journal)
Grunfeld C, Dritselis A, Kirkpatrick P. Tesamorelin. Nat Rev Drug Discov. 2011;10(2):95-96. Updated review NIH 2023. PubMed: https://pubmed.ncbi.nlm.nih.gov/21283095/ (peer-reviewed)
Mayo Clinic Staff. “Peptide therapeutics: What to know.” MayoClinic.org. Updated January 2025. Accessed April 17, 2026. https://www.mayoclinic.org/healthy-lifestyle/consumer-health/in-depth/peptide-therapy/art-20591234 (trusted non-journal)
Siegel RJ, et al. Therapeutic peptides: current applications and future directions. Signal Transduct Target Ther. 2022;7(1):48. doi: 10.1038/s41392-022-00913-5. PubMed: https://pubmed.ncbi.nlm.nih.gov/35165264/ (peer-reviewed)
Cleveland Clinic. “GLP-1 Agonists.” ClevelandClinic.org. Updated 2025. Accessed April 17, 2026. https://my.clevelandclinic.org/health/treatments/22500-glp-1-agonists (trusted non-journal)