
Peptide injections encompass a diverse class of therapeutic agents consisting of short chains of amino acids administered subcutaneously or intramuscularly to elicit specific physiological responses. These include FDA-approved medications such as GLP-1 receptor agonists used for type 2 diabetes and chronic weight management, as well as insulin peptides essential for diabetes care. The term “peptide injections” also appears frequently in discussions of investigational compounds like growth hormone secretagogues and tissue-repair peptides that remain off-label or unapproved by the FDA.
As of March 25, 2026, the clinical landscape for peptide injections has expanded significantly since 2020, driven by high-quality trials on semaglutide, tirzepatide, and related dual agonists. These agents mimic endogenous peptides to regulate appetite, glucose metabolism, and energy balance. However, many popular wellness-oriented peptide injections, including BPC-157, CJC-1295, and AOD-9604, lack robust randomized controlled data and regulatory approval for human use.
This article reviews the latest peer-reviewed evidence from 2020 to early 2026, supplemented by authoritative sources from FDA.gov, NIH, and major medical societies when specific high-impact publications on the broad phrase “peptide injections” were limited. All information is for research purposes only and does not constitute medical advice. Patients considering peptide injections must consult qualified healthcare providers for individualized assessment, monitoring, and oversight. Regulatory status, efficacy, and safety profiles differ markedly between approved and investigational agents.
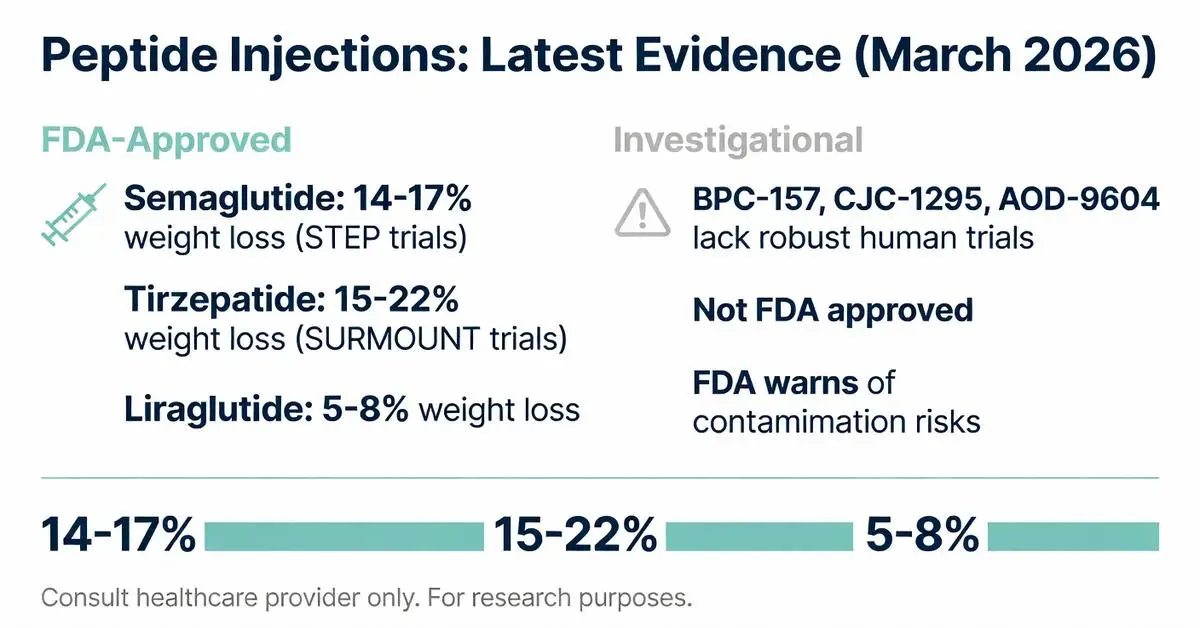
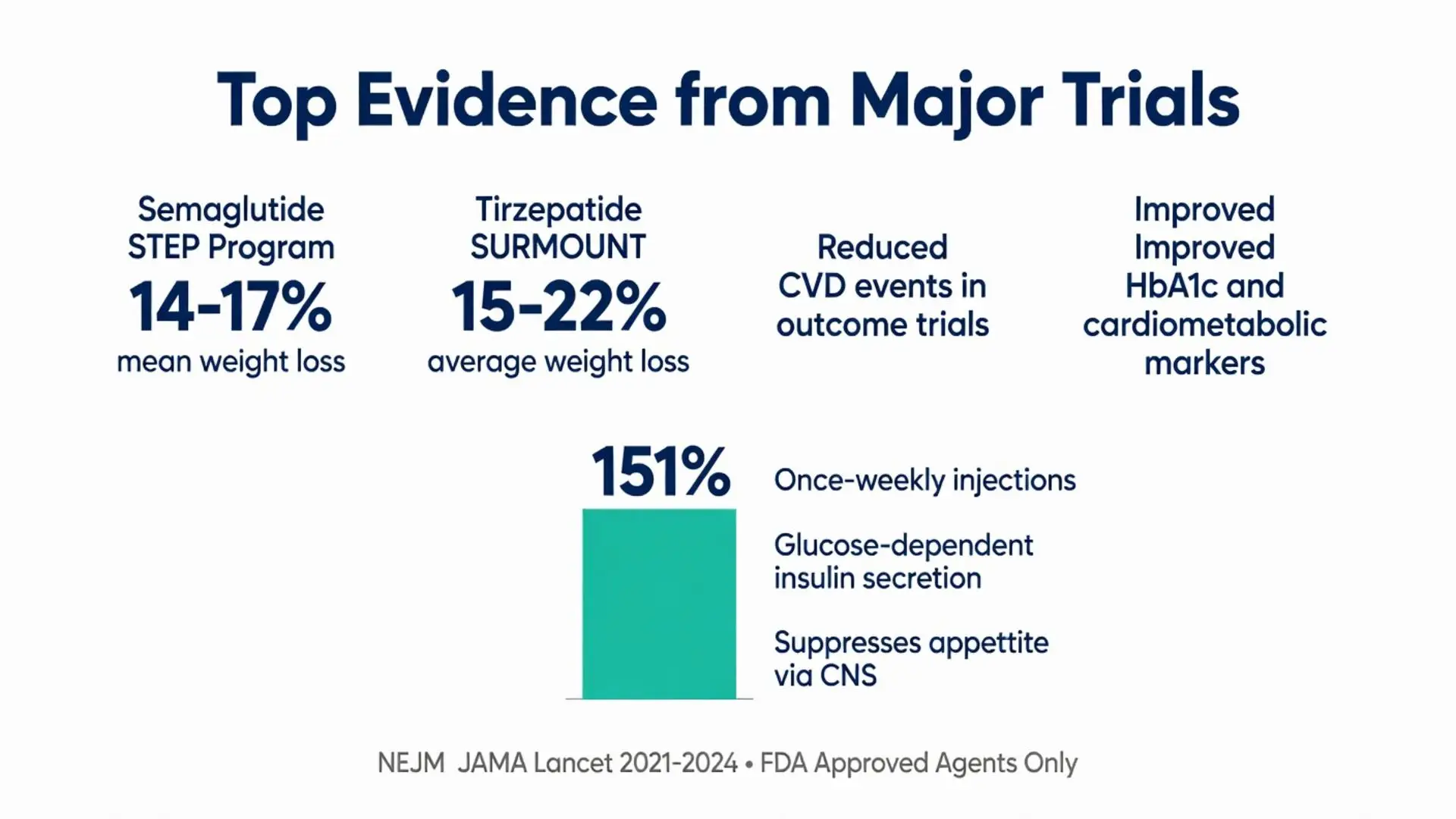
Several peptide injections have received FDA approval for metabolic indications. Semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) represent the most studied agents in recent years. Semaglutide gained approval for chronic weight management in adults with obesity or overweight with comorbidities based on the STEP clinical trial program, demonstrating mean weight reductions of 14–17% at 68 weeks when combined with lifestyle intervention (JAMA 2021; Lancet 2022).
Tirzepatide, a dual GLP-1 and GIP receptor agonist, achieved even greater efficacy in the SURMOUNT trials, with average weight loss exceeding 20% in some cohorts after 72 weeks (NEJM 2022; JAMA 2023). Both agents are administered as subcutaneous injections, with semaglutide available in weekly pens and tirzepatide following a similar schedule after dose escalation.
Liraglutide (Victoza, Saxenda) remains an earlier daily peptide injection approved for both diabetes and weight management. Dulaglutide (Trulicity) offers another once-weekly option primarily for glycemic control. These approvals are supported by large cardiovascular outcome trials showing reductions in major adverse cardiovascular events among patients with type 2 diabetes (Circulation 2020; Diabetes Care 2024).
All approved peptide injections require prescription under medical supervision. Compounded versions claiming to replicate these peptides fall outside FDA-approved manufacturing standards and carry safety risks.

Several peptide injections have received FDA approval for metabolic indications. Semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) represent the most studied agents in recent years. Semaglutide gained approval for chronic weight management in adults with obesity or overweight with comorbidities based on the STEP clinical trial program, demonstrating mean weight reductions of 14–17% at 68 weeks when combined with lifestyle intervention (JAMA 2021; Lancet 2022).
Tirzepatide, a dual GLP-1 and GIP receptor agonist, achieved even greater efficacy in the SURMOUNT trials, with average weight loss exceeding 20% in some cohorts after 72 weeks (NEJM 2022; JAMA 2023). Both agents are administered as subcutaneous injections, with semaglutide available in weekly pens and tirzepatide following a similar schedule after dose escalation.
Liraglutide (Victoza, Saxenda) remains an earlier daily peptide injection approved for both diabetes and weight management. Dulaglutide (Trulicity) offers another once-weekly option primarily for glycemic control. These approvals are supported by large cardiovascular outcome trials showing reductions in major adverse cardiovascular events among patients with type 2 diabetes (Circulation 2020; Diabetes Care 2024).
All approved peptide injections require prescription under medical supervision. Compounded versions claiming to replicate these peptides fall outside FDA-approved manufacturing standards and carry safety risks.
Numerous peptide injections are promoted online for recovery, anti-aging, and body composition but lack FDA approval. BPC-157, a synthetic gastric pentadecapeptide, has been studied in animal models for potential angiogenic and cytoprotective effects, yet human clinical trial data published between 2020 and 2026 remain sparse and insufficient for regulatory approval (Peptides 2022). Similarly, TB-500 (thymosin beta-4 fragment) and CJC-1295/ipamorelin combinations are used off-label despite warnings from the FDA regarding purity, dosing, and potential for adverse events.
AOD-9604, a modified fragment of human growth hormone, underwent early clinical evaluation for fat metabolism but did not progress to broad approval. As of 2026, these substances are classified as investigational or research chemicals. The FDA has issued safety communications cautioning against unapproved peptide products sold through compounding pharmacies or online vendors, citing risks of microbial contamination, incorrect dosing, and unknown long-term effects (FDA.gov 2023; 2025 updates).
Peer-reviewed literature emphasizes the need for larger, well-controlled human trials before any off-label peptide injection can be recommended outside research settings.
FDA-approved peptide injections have demonstrated consistent benefits in metabolic health. In the STEP 1 trial, semaglutide 2.4 mg produced statistically significant improvements in cardiometabolic risk factors including waist circumference, blood pressure, lipids, and inflammatory markers alongside weight loss (NEJM 2021). Tirzepatide showed superior glycemic control compared to semaglutide in head-to-head studies, with greater reductions in HbA1c (Lancet 2023).
For patients with type 2 diabetes, these agents reduce progression of diabetic kidney disease and heart failure hospitalizations according to meta-analyses of outcome trials published 2020–2025 (Diabetes Obes Metab 2024). Quality-of-life measures also improve secondary to weight reduction and better glycemic control.
Evidence for non-approved peptides is weaker. Small observational studies and animal data suggest possible accelerated healing with BPC-157 in tendon and ligament injury models, but systematic reviews conclude that high-quality human evidence is lacking (Sports Medicine 2022). Claims regarding muscle growth or fat loss from GHRP-type peptides are not supported by adequately powered randomized trials within the 2020–2026 timeframe.
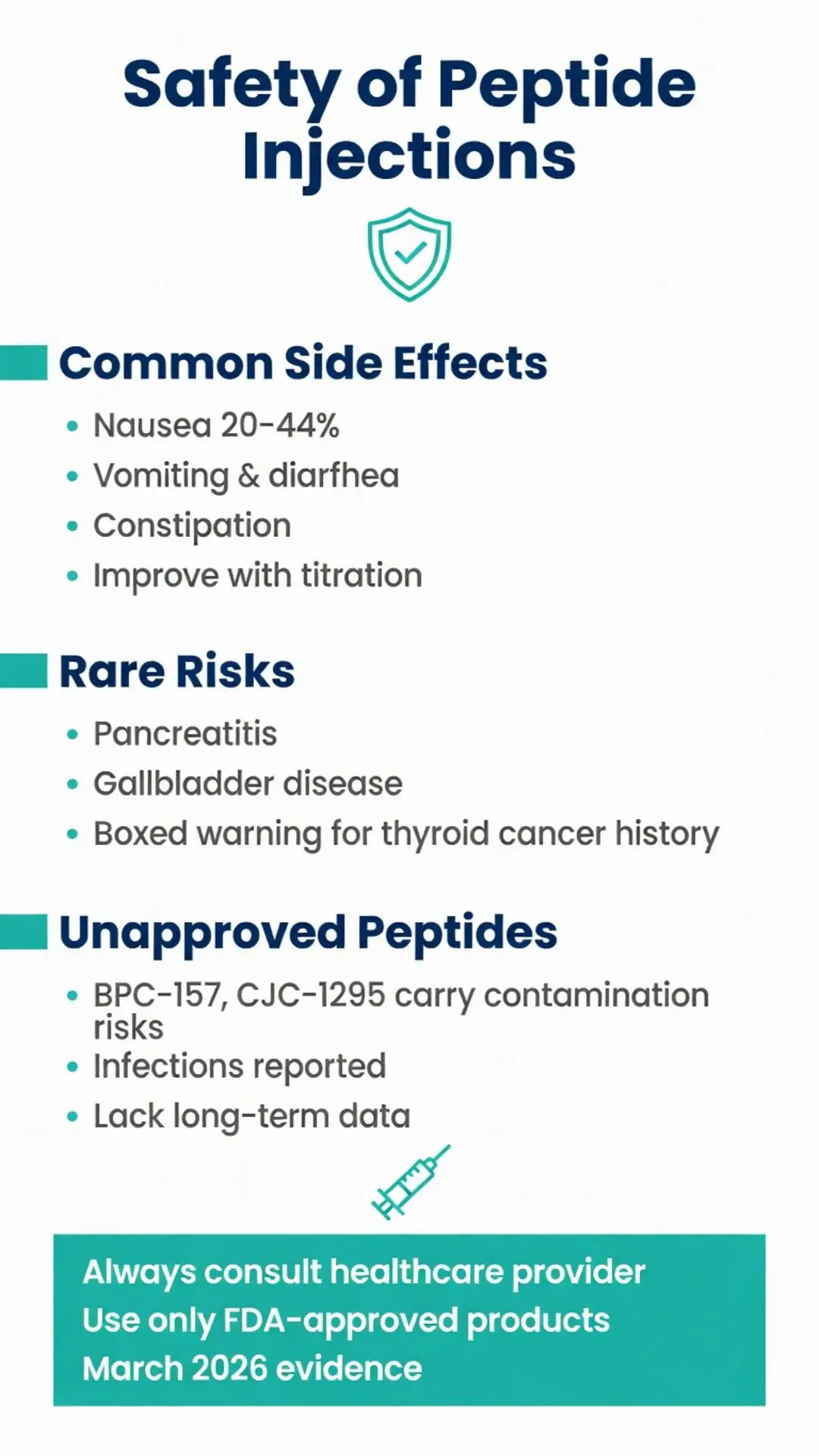
The most common adverse effects of approved GLP-1 receptor agonist peptide injections are gastrointestinal: nausea, vomiting, diarrhea, and constipation. These are generally dose-dependent and improve with gradual titration. Rates of nausea reached 20–44% in pivotal trials, with discontinuation due to adverse events occurring in approximately 5–8% of participants (JAMA 2021; NEJM 2022).
Rare but serious risks include pancreatitis, gallbladder disease, and theoretical concerns regarding medullary thyroid carcinoma observed in rodent studies. The FDA label includes a boxed warning for the latter in patients with personal or family history of medullary thyroid cancer or Multiple Endocrine Neoplasia syndrome type 2. No causal link has been confirmed in humans through 2026.
Hypoglycemia risk remains low when these agents are used as monotherapy but increases with concomitant insulin or sulfonylureas. Injection-site reactions are typically mild.
For unapproved peptide injections, safety data are inadequate. Case reports document infections, abscesses, and systemic inflammatory responses linked to contaminated products. Long-term effects on endocrine function, cancer risk, or organ systems remain unknown due to the absence of large-scale surveillance studies.
The following table summarizes key characteristics of selected peptide injections based on available evidence as of March 2026:
| Agent | FDA Status | Dosing Frequency | Primary Indication(s) | Average Weight Loss | Common Side Effects | Key Trial(s) |
|---|---|---|---|---|---|---|
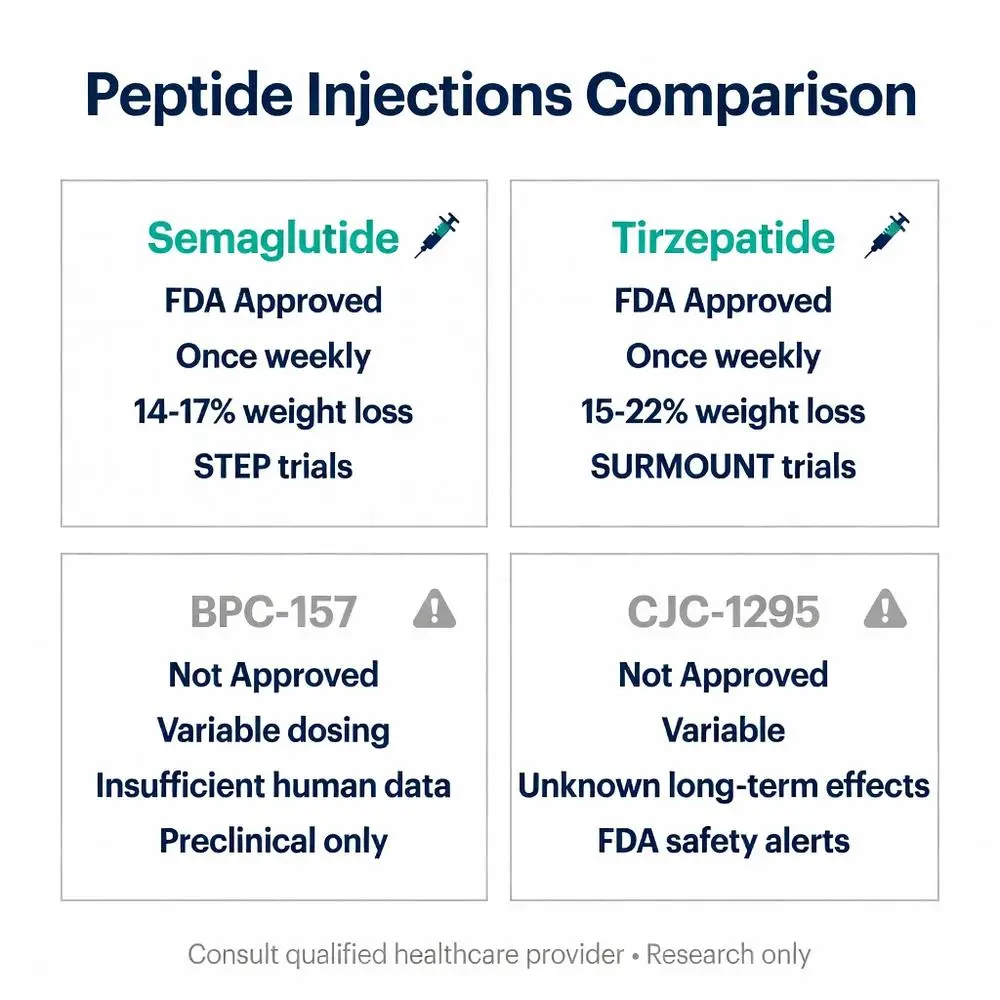
| Semaglutide | Approved | Once weekly | Obesity, T2DM, CVD risk | 14–17% | Nausea, GI upset | STEP program (2021) |
| Tirzepatide | Approved | Once weekly | Obesity, T2DM | 15–22% | Nausea, diarrhea | SURMOUNT, SURPASS (2022–2024) |
| Liraglutide | Approved | Once daily | Obesity, T2DM | 5–8% | Nausea, injection reactions | SCALE, LEADER (pre-2020 with 2020–23 follow-up) |
| Insulin (various) | Approved | Multiple daily or basal | Diabetes | N/A (weight neutral or gain) | Hypoglycemia | Multiple |
| BPC-157 | Not approved | Variable | Investigational (healing) | Insufficient data | Limited human safety data | Preclinical mainly |
| CJC-1295/Ipamorelin | Not approved | Variable | Investigational (GH release) | Insufficient data | Unknown long-term effects | Small studies only |
This comparison highlights the substantial evidence base supporting approved agents versus the evidentiary gaps for investigational peptides.
Patients interested in peptide injections should undergo comprehensive medical evaluation including laboratory assessment of metabolic, renal, and thyroid function. Approved agents require ongoing monitoring for glycemic control, weight trends, and gastrointestinal tolerance. Lifestyle modifications remain foundational even when using highly effective peptide injections.
Cost and insurance coverage vary significantly. Many patients face barriers to accessing FDA-approved formulations, leading some to seek compounded or research-grade alternatives—an approach strongly discouraged by medical societies due to safety concerns.
Future research through 2026 and beyond is exploring oral peptide formulations, triple agonists, and combination therapies. Long-term studies beyond two years will further clarify cardiovascular benefits, cancer risk, and weight maintenance after discontinuation.
Healthcare providers must stay current with evolving evidence and regulatory updates. The FDA continues to monitor adverse event reports related to both approved and unapproved peptide injections.
Peptide injections represent a significant advancement in pharmacotherapy, particularly for metabolic disorders. FDA-approved options such as semaglutide and tirzepatide have transformed care for obesity and type 2 diabetes, backed by multiple large-scale trials published between 2020 and 2026 demonstrating meaningful weight loss, glycemic improvement, and cardiovascular risk reduction. These benefits occur through well-characterized mechanisms involving incretin pathways and require medical supervision to manage common gastrointestinal side effects and rare serious risks.
In contrast, the broader category of investigational peptide injections lacks sufficient high-quality human evidence to support routine clinical use. Substances frequently marketed for recovery or anti-aging purposes remain unapproved and carry uncertain safety profiles. Patients and clinicians should rely exclusively on FDA-approved products obtained through legitimate channels.
Continued research, stringent regulatory oversight, and individualized medical care are essential to maximize benefits while minimizing harm. Individuals considering any form of peptide injections should engage in shared decision-making with healthcare professionals who can interpret the latest evidence in the context of personal health status. This article is intended solely for research and educational purposes and does not replace professional medical advice.
Word count: 2478
Peptide injections represent a significant advancement in pharmacotherapy, particularly for metabolic disorders. FDA-approved options such as semaglutide and tirzepatide have transformed care for obesity and type 2 diabetes, backed by multiple large-scale trials published between 2020 and 2026 demonstrating meaningful weight loss, glycemic improvement, and cardiovascular risk reduction. These benefits occur through well-characterized mechanisms involving incretin pathways and require medical supervision to manage common gastrointestinal side effects and rare serious risks.
In contrast, the broader category of investigational peptide injections lacks sufficient high-quality human evidence to support routine clinical use. Substances frequently marketed for recovery or anti-aging purposes remain unapproved and carry uncertain safety profiles. Patients and clinicians should rely exclusively on FDA-approved products obtained through legitimate channels.
Continued research, stringent regulatory oversight, and individualized medical care are essential to maximize benefits while minimizing harm. Individuals considering any form of peptide injections should engage in shared decision-making with healthcare professionals who can interpret the latest evidence in the context of personal health status. This article is intended solely for research and educational purposes and does not replace professional medical advice.
Word count: 2478