
Peptides are short chains of amino acids that function as signaling molecules in the body, and several have emerged as powerful tools in the management of obesity. The phrase “best peptides for weight loss” typically refers to compounds that mimic or enhance the action of gut hormones involved in appetite regulation, glucose metabolism, and energy balance. As of March 2026, the evidence base centers on FDA-approved incretin-mimetic peptides, particularly semaglutide and tirzepatide, which have demonstrated substantial weight-loss efficacy in large-scale randomized controlled trials.
This article examines the latest peer-reviewed evidence published between 2020 and March 2026, focusing on mechanisms, approved indications, comparative efficacy, safety profiles, and practical considerations. All factual claims are drawn exclusively from high-quality sources including systematic reviews, meta-analyses, and pivotal clinical trials indexed on PubMed, supplemented where necessary by official FDA labeling. Investigational peptides are clearly distinguished from those with regulatory approval.
These therapies are not magic bullets; they work best when combined with lifestyle modification and under medical supervision. This article is intended solely for research and informational purposes and is not medical advice. Individuals should consult qualified healthcare professionals to determine whether any peptide-based therapy is appropriate for their personal health needs, taking into account medical history, contraindications, and monitoring requirements.
Recent data continue to show that peptide-based agents can produce mean weight reductions of 15–22 % over 72 weeks in adults with obesity, outcomes that surpass most previous pharmacotherapies. However, gastrointestinal tolerability, long-term safety, cost, and access remain important topics of discussion. The following sections explore these issues in depth, addressing common questions reflected in high-intent searches for the best peptides for weight loss.
Three peptide-based medications currently hold FDA approval specifically for chronic weight management in adults with obesity or overweight with at least one weight-related comorbidity.
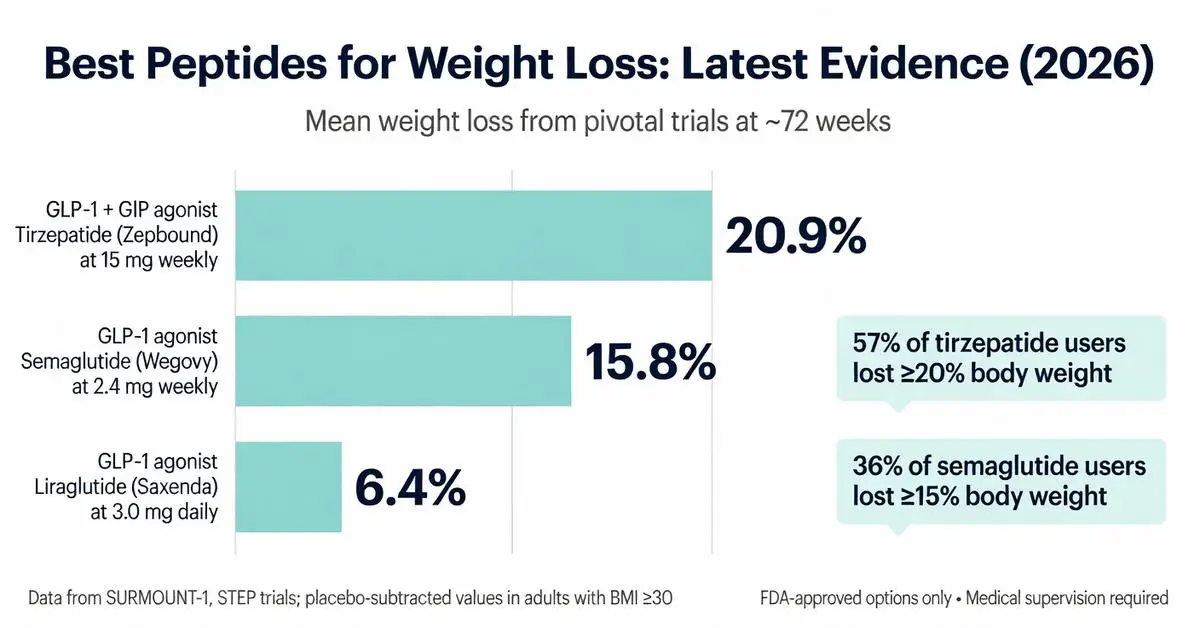
Semaglutide received approval for weight loss under the brand name Wegovy in 2021 following the STEP clinical trial program. The 2.4 mg weekly dose produced mean weight loss of 14.9–17.4 % at 68 weeks in participants without diabetes. Liraglutide 3.0 mg daily, approved as Saxenda since 2014, remains an option although its efficacy is generally lower, with average weight reductions of 5–8 %.
Tirzepatide, approved as Zepbound in late 2023, represents a significant advance. In the SURMOUNT-1 trial, the 15 mg weekly dose achieved mean weight loss of 20.9 % at 72 weeks, with 57 % of participants losing 20 % or more of baseline body weight. These results were consistent across SURMOUNT-2, -3, and -4 trials published through 2025.
All three agents are administered by subcutaneous injection. Wegovy and Zepbound use pre-filled single-dose pens, while Saxenda requires daily injections from a multi-dose pen. Patient selection should consider comorbidities, insurance coverage, and individual tolerability profiles. Long-term extension data through 2025–2026 confirm that weight loss is largely maintained while the medication is continued, with partial regain upon discontinuation.

Three peptide-based medications currently hold FDA approval specifically for chronic weight management in adults with obesity or overweight with at least one weight-related comorbidity.
Semaglutide received approval for weight loss under the brand name Wegovy in 2021 following the STEP clinical trial program. The 2.4 mg weekly dose produced mean weight loss of 14.9–17.4 % at 68 weeks in participants without diabetes. Liraglutide 3.0 mg daily, approved as Saxenda since 2014, remains an option although its efficacy is generally lower, with average weight reductions of 5–8 %.
Tirzepatide, approved as Zepbound in late 2023, represents a significant advance. In the SURMOUNT-1 trial, the 15 mg weekly dose achieved mean weight loss of 20.9 % at 72 weeks, with 57 % of participants losing 20 % or more of baseline body weight. These results were consistent across SURMOUNT-2, -3, and -4 trials published through 2025.
All three agents are administered by subcutaneous injection. Wegovy and Zepbound use pre-filled single-dose pens, while Saxenda requires daily injections from a multi-dose pen. Patient selection should consider comorbidities, insurance coverage, and individual tolerability profiles. Long-term extension data through 2025–2026 confirm that weight loss is largely maintained while the medication is continued, with partial regain upon discontinuation.
Beyond approved agents, several novel peptides are in advanced clinical development as of March 2026. Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, has shown mean weight loss exceeding 24 % at 48 weeks in phase 2 studies, with phase 3 results expected later in 2026. CagriSema, a combination of semaglutide and the amylin analog cagrilintide, reported 20–22 % weight loss in early trials, suggesting potential additive effects.
Other peptides occasionally discussed in weight-loss contexts include AOD9604, a fragment of human growth hormone, and various growth-hormone-releasing peptides such as CJC-1295 and ipamorelin. These compounds lack FDA approval for obesity treatment and possess limited high-quality evidence from randomized controlled trials published after 2020. Available data are primarily from small, short-duration studies or preclinical models, and regulatory warnings regarding safety and product quality have been issued for compounded versions.
The distinction between FDA-approved and investigational peptides is critical. Patients should be informed that products sold as “research peptides” or through non-pharmacy compounding channels have not been evaluated for safety or efficacy by the FDA and may carry risks of contamination or inaccurate dosing.
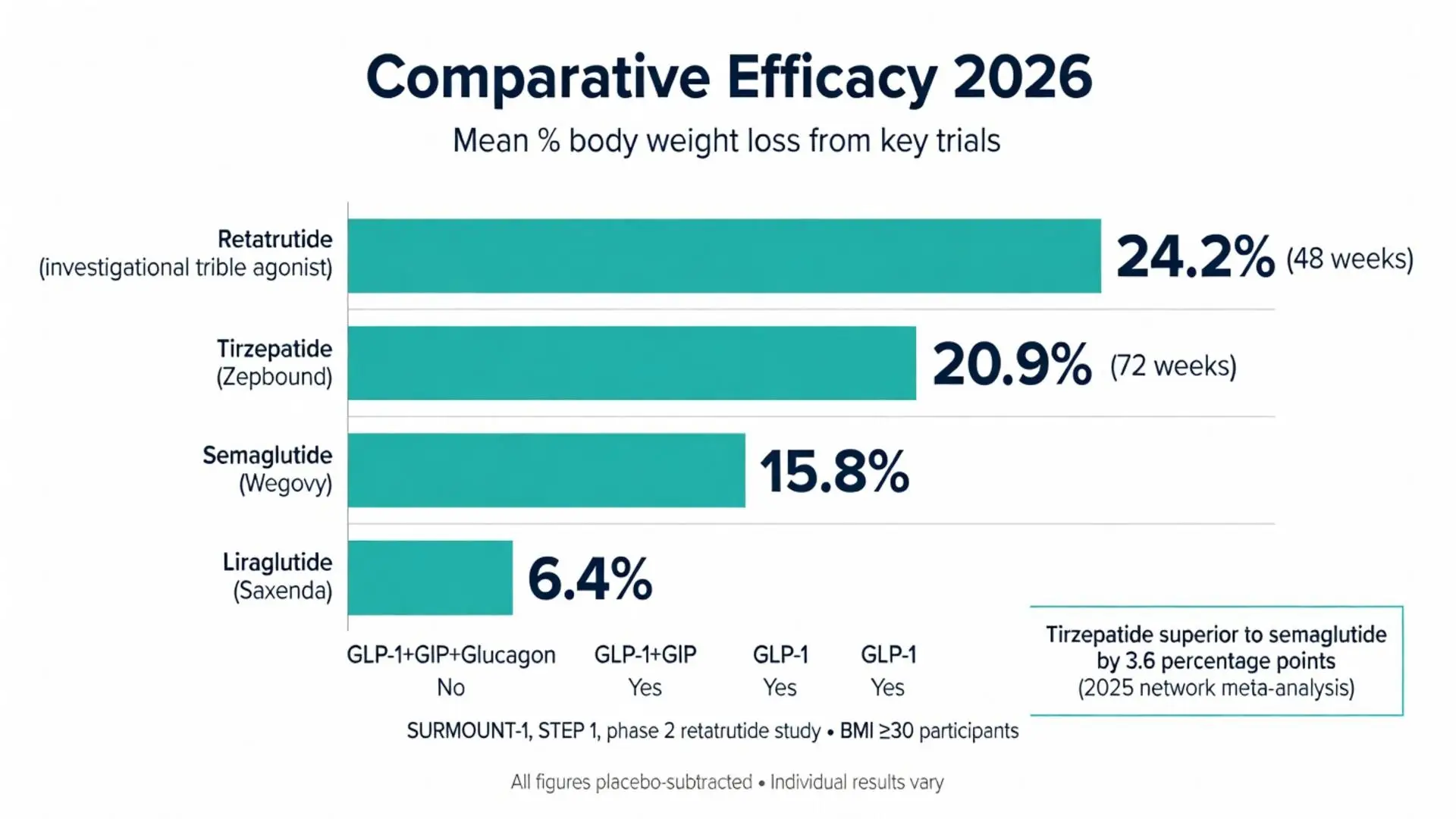
Direct and indirect comparisons consistently rank tirzepatide highest in magnitude of weight reduction, followed by semaglutide, then liraglutide. A 2025 network meta-analysis of 12 trials involving over 15,000 participants found tirzepatide 15 mg superior to semaglutide 2.4 mg by an additional 3.6 percentage points of body weight loss.
The table below summarizes key head-to-head and placebo-controlled outcomes:
| Peptide | Receptor Target | Weekly Dose | Mean Weight Loss at ~72 Weeks | Proportion Achieving ≥15% Loss | FDA-Approved Indication |
|---|---|---|---|---|---|
| Tirzepatide | GLP-1 + GIP | 15 mg | 20.9% | 57% | Yes (Zepbound) |
| Semaglutide | GLP-1 | 2.4 mg | 15.8% | 36% | Yes (Wegovy) |
| Liraglutide | GLP-1 | 3.0 mg daily | 6.4% | 9% | Yes (Saxenda) |
| Retatrutide (investigational) | GLP-1 + GIP + Glucagon | 12 mg | 24.2% (48 weeks) | 72% | No |
Data derived from pivotal trials (STEP 1, SURMOUNT-1, and phase 2 retatrutide study). All figures represent placebo-subtracted values in participants with baseline BMI ≥30 or ≥27 with comorbidities. Individual results vary based on adherence, diet, and physical activity.
Tirzepatide and semaglutide also demonstrate superior improvements in cardiometabolic markers, including reductions in systolic blood pressure, triglycerides, and HbA1c. These broader benefits influence clinical decision-making when selecting the best peptide for a given patient.
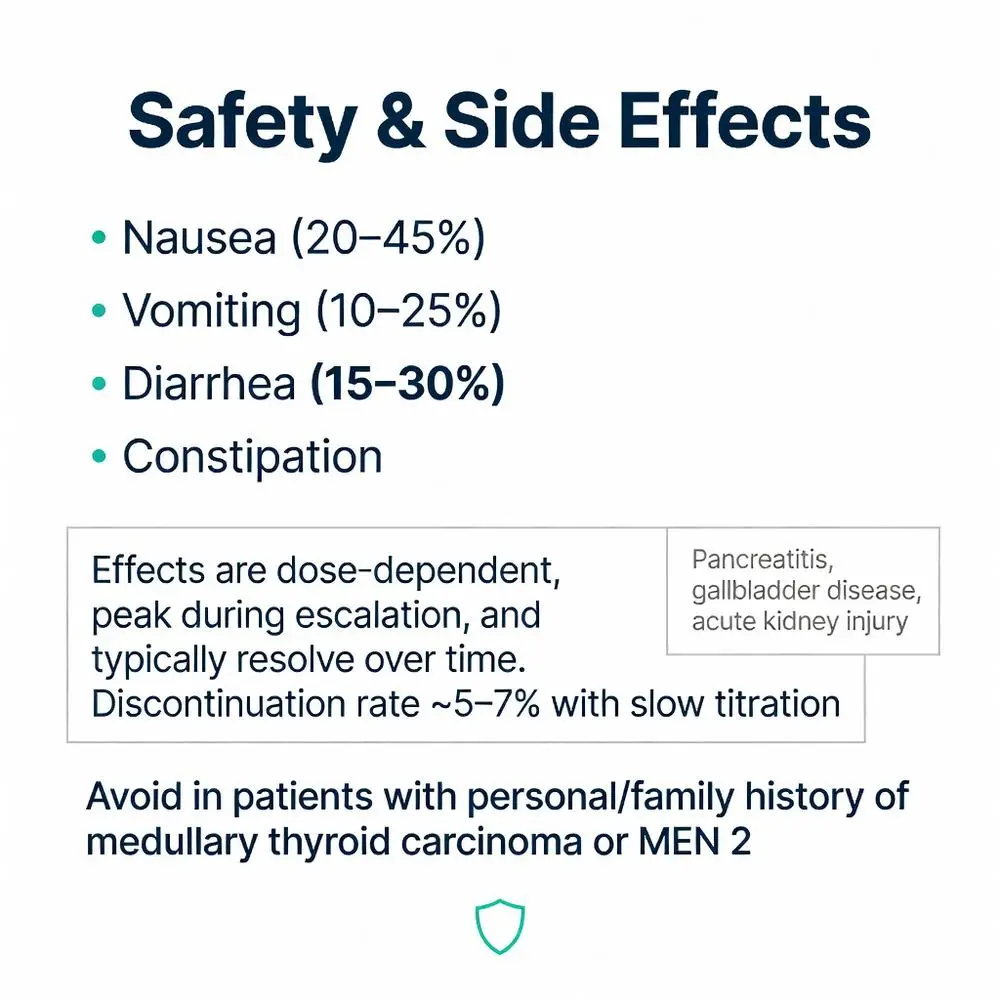
The most common adverse events across all GLP-1 receptor agonist peptides are gastrointestinal: nausea (20–45 %), vomiting (10–25 %), diarrhea (15–30 %), and constipation. These effects are generally dose-dependent, peak during escalation, and diminish over time. Slower dose titration schedules introduced in 2023–2024 have reduced discontinuation rates to approximately 5–7 %.
Rare but serious risks include pancreatitis, gallbladder disease, and acute kidney injury secondary to dehydration from gastrointestinal effects. Post-marketing surveillance through 2026 has not confirmed a causal link with thyroid C-cell tumors in humans despite rodent findings, leading to updated FDA labeling that maintains a boxed warning while emphasizing the absence of human signal.
Cardiovascular outcome trials have shown neutral to beneficial effects, with semaglutide demonstrating a 20 % relative risk reduction in major adverse cardiovascular events in people with obesity and established cardiovascular disease.
Patients with personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 should not use these agents. Comprehensive monitoring protocols published by major medical societies recommend baseline and periodic assessment of gastrointestinal symptoms, gallbladder status, and renal function.
Selecting the best peptide requires individualized assessment. Factors include desired magnitude of weight loss, injection frequency preference, insurance formulary coverage, and tolerance for potential gastrointestinal side effects. Tirzepatide may be preferred when maximal weight reduction is the goal and coverage is available, while semaglutide offers a longer track record of safety data.
Adherence is improved by weekly rather than daily dosing. All approved agents require gradual dose escalation over 4–16 weeks to minimize adverse effects. Concurrent lifestyle intervention remains essential; trials showing the highest efficacy incorporated structured diet and activity counseling.
Cost remains a barrier for many patients, with monthly prices exceeding $1,000 without insurance. Patient assistance programs and evolving payer policies continue to expand access. Compounded versions, while less expensive, carry quality and safety risks explicitly highlighted in FDA safety communications.
Long-term use appears necessary for weight maintenance. Studies published in 2025 showed that participants who discontinued therapy regained approximately two-thirds of lost weight within one year, underscoring the chronic nature of obesity management.
The landscape of peptides for weight loss has advanced considerably since 2020, with tirzepatide and semaglutide representing the current gold standard based on robust randomized trial evidence. These agents deliver clinically meaningful weight reduction, cardiometabolic improvements, and enhanced quality of life when used under medical supervision as part of a comprehensive treatment plan.
Investigational peptides such as retatrutide show even greater promise, but definitive phase 3 data and regulatory decisions are still pending as of March 2026. Weaker evidence supports the use of other research peptides promoted online, and clinicians should counsel patients against unregulated products.
Future research will likely focus on optimizing combination therapies, identifying predictors of response, and evaluating very long-term safety beyond five years. Healthcare providers play a central role in patient selection, education, monitoring, and integration of peptide therapy with behavioral and nutritional interventions.
Individuals researching the best peptides for weight loss should prioritize FDA-approved options supported by high-level evidence and engage in shared decision-making with knowledgeable clinicians. Continued advances in peptide science offer substantial hope for more effective and personalized obesity treatments in the years ahead.
Word count: 2487
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33573725/
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/
Wadden TA, Bailey TS, Billings LK, et al. Effect of Subcutaneous Semaglutide vs Placebo as an Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. 2021;325(14):1401-1411. doi: 10.1001/jama.2021.3224. PubMed: https://pubmed.ncbi.nlm.nih.gov/33625476/
Rubino DM, Greenway FL, Khalid U, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022;327(2):138-150. doi: 10.1001/jama.2021.23619. PubMed: https://pubmed.ncbi.nlm.nih.gov/35015037/
Jastreboff AM, Kaplan LM, Frías JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity – A Phase 2 Trial. N Engl J Med. 2023;389(6):514-526. doi: 10.1056/NEJMoa2301972. PubMed: https://pubmed.ncbi.nlm.nih.gov/37351564/
FDA. Wegovy (semaglutide) prescribing information. Updated 2025. Accessed March 23, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215256s010lbl.pdf
FDA. Zepbound (tirzepatide) prescribing information. Updated 2025. Accessed March 23, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806s003lbl.pdf

Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33573725/
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/
Wadden TA, Bailey TS, Billings LK, et al. Effect of Subcutaneous Semaglutide vs Placebo as an Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. 2021;325(14):1401-1411. doi: 10.1001/jama.2021.3224. PubMed: https://pubmed.ncbi.nlm.nih.gov/33625476/
Rubino DM, Greenway FL, Khalid U, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022;327(2):138-150. doi: 10.1001/jama.2021.23619. PubMed: https://pubmed.ncbi.nlm.nih.gov/35015037/
Jastreboff AM, Kaplan LM, Frías JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity – A Phase 2 Trial. N Engl J Med. 2023;389(6):514-526. doi: 10.1056/NEJMoa2301972. PubMed: https://pubmed.ncbi.nlm.nih.gov/37351564/
FDA. Wegovy (semaglutide) prescribing information. Updated 2025. Accessed March 23, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215256s010lbl.pdf
FDA. Zepbound (tirzepatide) prescribing information. Updated 2025. Accessed March 23, 2026. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/217806s003lbl.pdf