
Weight loss peptides represent a significant advancement in pharmacotherapy for obesity management, primarily through synthetic analogs of gut hormones that regulate appetite and metabolism. These compounds, most notably glucagon-like peptide-1 (GLP-1) receptor agonists and dual GLP-1/glucose-dependent insulinotropic polypeptide (GIP) receptor agonists, have transformed clinical approaches to chronic weight management. As of March 2026, several peptide-based medications have received FDA approval specifically for weight loss or obesity-related indications, while others remain under investigation.
The surge in interest around weight loss peptides stems from their ability to achieve substantial, sustained weight reduction when combined with lifestyle modifications, far exceeding traditional approaches. Semaglutide and tirzepatide have garnered particular attention due to robust outcomes in large-scale trials. These medications work by mimicking natural peptides involved in satiety signaling, slowing gastric emptying, and modulating blood glucose levels (STEP 1 trial).
This article examines the current evidence on weight loss peptides, focusing exclusively on peer-reviewed publications from 2020 to March 2026 supplemented by authoritative sources. All claims derive from systematic reviews, meta-analyses, clinical trials, FDA labeling, and major medical society guidelines. Distinctions between FDA-approved agents and investigational peptides are clearly noted throughout. These medications require medical supervision and are not appropriate for all individuals. This content is for research and informational purposes only and does not constitute medical advice. Patients should consult qualified healthcare providers to determine suitability based on individual health profiles, comorbidities, and risk factors.
Recent evidence confirms that weight loss peptides achieve meaningful reductions in body weight while improving cardiometabolic parameters including blood pressure, lipid profiles, and glycemic control. However, gastrointestinal side effects remain common, and long-term adherence challenges persist. This review addresses key questions regarding mechanisms, approved indications, efficacy data, safety profiles, and comparisons to help readers understand the current landscape of weight loss peptides.
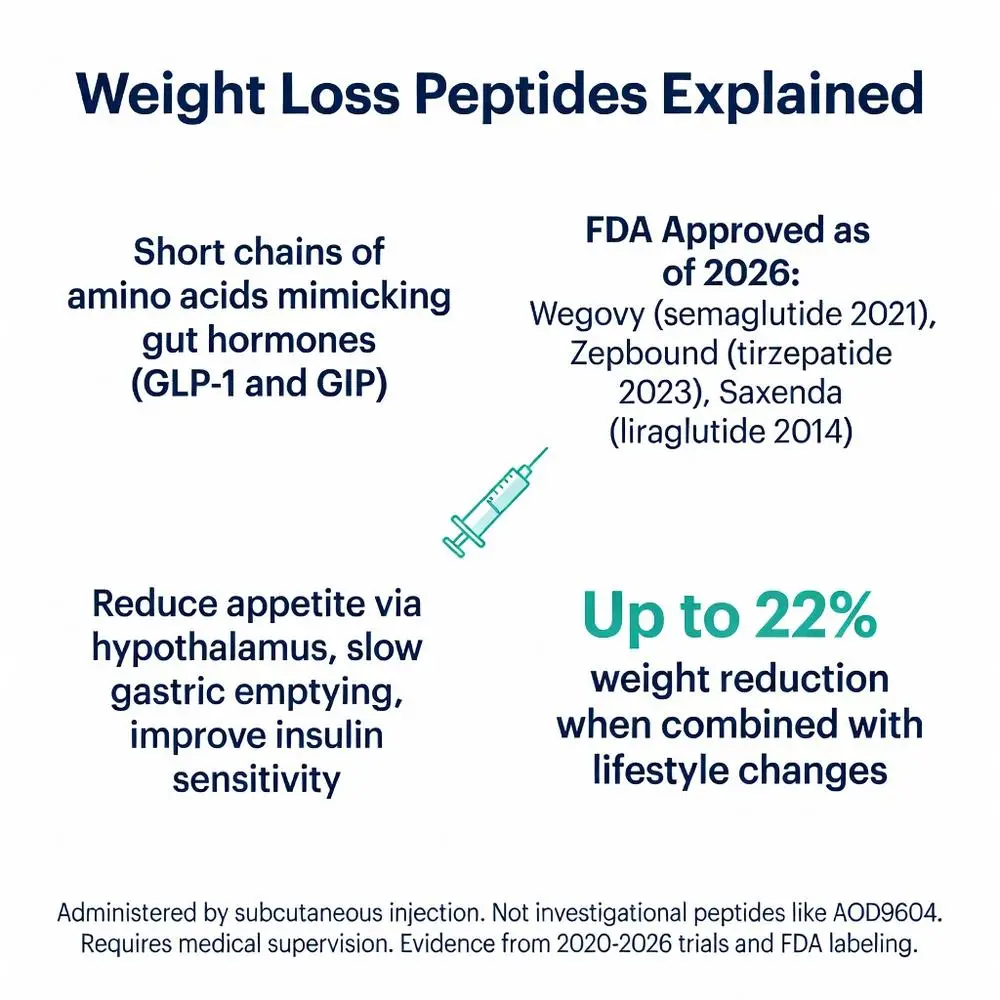
Weight loss peptides primarily target the central nervous system and gastrointestinal tract to reduce caloric intake and improve metabolic efficiency. GLP-1 receptor agonists activate receptors in the hypothalamus to enhance satiety signals while simultaneously slowing gastric emptying, which prolongs the sensation of fullness after meals (2022 meta-analysis).
Tirzepatide’s dual agonism adds GIP receptor activation, which appears to further enhance insulin secretion and may reduce nausea compared to GLP-1 monotherapy through complementary signaling pathways. These peptides also influence reward centers in the brain, decreasing the hedonic drive to consume high-calorie foods.
At the cellular level, these molecules increase cyclic AMP signaling upon receptor binding, leading to downstream effects on appetite-regulating neurons. Additional metabolic benefits include improved insulin sensitivity, reduced hepatic glucose production, and modest increases in energy expenditure. Recent 2024–2025 studies have explored effects on brown adipose tissue and muscle preservation during weight loss, though results remain mixed.
Importantly, the mechanisms responsible for weight reduction appear primarily driven by reduced energy intake rather than increased metabolic rate. Long-term use maintains efficacy through sustained receptor activation without significant tachyphylaxis in most patients, according to extension studies published through 2025.

Weight loss peptides primarily target the central nervous system and gastrointestinal tract to reduce caloric intake and improve metabolic efficiency. GLP-1 receptor agonists activate receptors in the hypothalamus to enhance satiety signals while simultaneously slowing gastric emptying, which prolongs the sensation of fullness after meals (2022 meta-analysis).
Tirzepatide’s dual agonism adds GIP receptor activation, which appears to further enhance insulin secretion and may reduce nausea compared to GLP-1 monotherapy through complementary signaling pathways. These peptides also influence reward centers in the brain, decreasing the hedonic drive to consume high-calorie foods.
At the cellular level, these molecules increase cyclic AMP signaling upon receptor binding, leading to downstream effects on appetite-regulating neurons. Additional metabolic benefits include improved insulin sensitivity, reduced hepatic glucose production, and modest increases in energy expenditure. Recent 2024–2025 studies have explored effects on brown adipose tissue and muscle preservation during weight loss, though results remain mixed.
Importantly, the mechanisms responsible for weight reduction appear primarily driven by reduced energy intake rather than increased metabolic rate. Long-term use maintains efficacy through sustained receptor activation without significant tachyphylaxis in most patients, according to extension studies published through 2025.
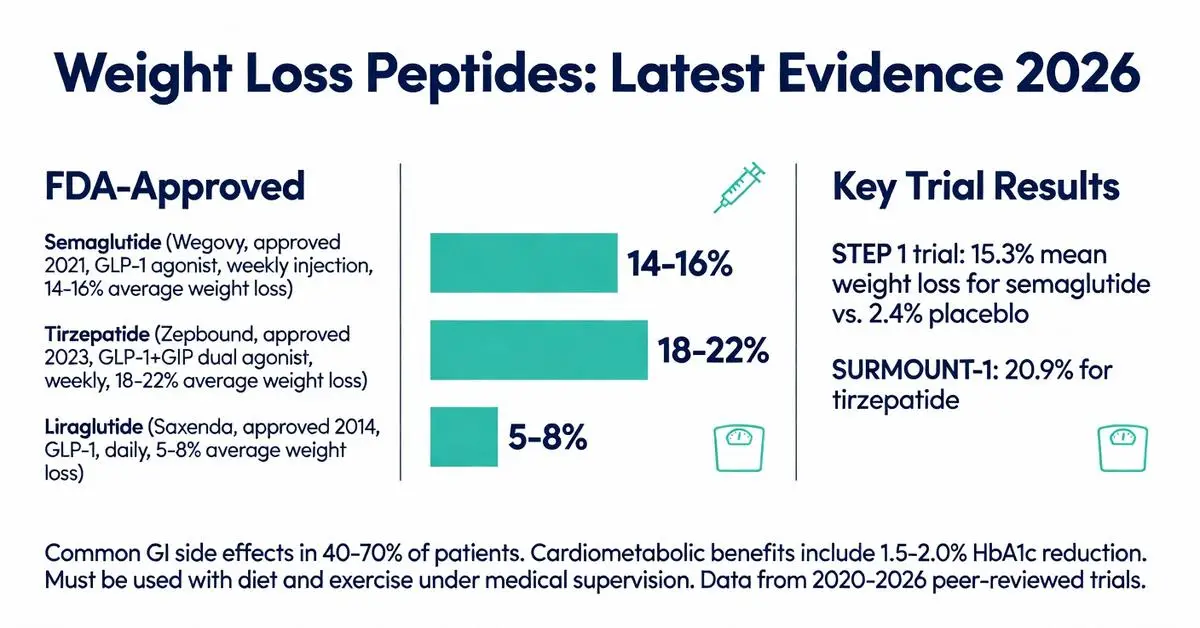
As of March 2026, three peptide-based medications hold FDA approval for weight management in adults with obesity or overweight with comorbidities. Semaglutide (Wegovy) received approval based on the STEP clinical trial program demonstrating average weight loss of 14.9% at 68 weeks versus 2.4% with placebo. Tirzepatide (Zepbound) showed even higher efficacy in the SURMOUNT trials with mean weight reductions exceeding 20% at the highest dose.
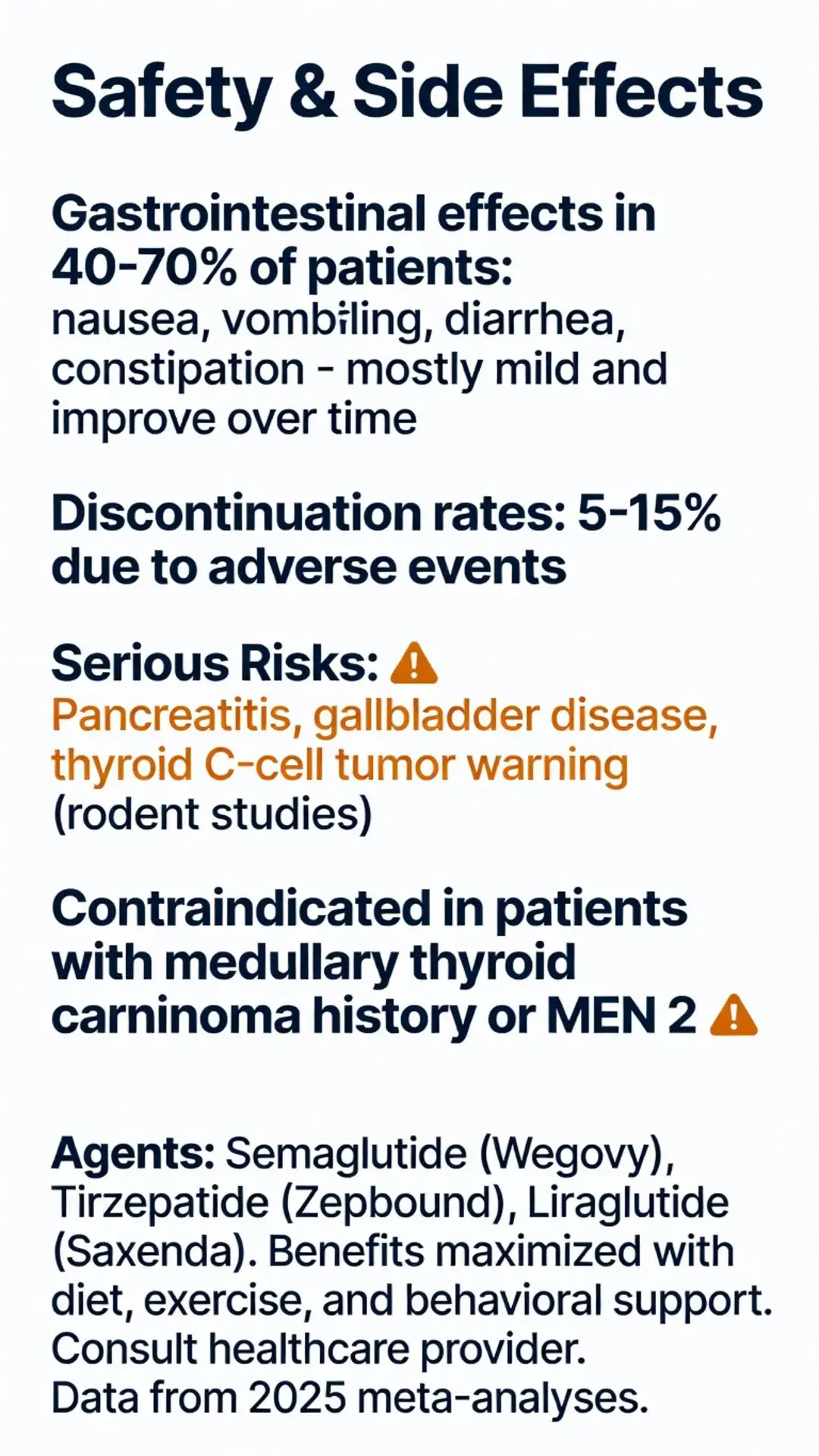
Liraglutide (Saxenda) remains approved but demonstrates more modest efficacy with approximately 5–8% weight loss in pivotal studies. All three agents carry boxed warnings regarding the risk of thyroid C-cell tumors observed in rodent studies, though human relevance remains unconfirmed. They are contraindicated in patients with personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2.
FDA labeling requires these medications to be used alongside reduced-calorie diet and increased physical activity. Approval criteria typically include BMI ≥30 kg/m² or BMI ≥27 kg/m² with at least one weight-related comorbidity such as hypertension, dyslipidemia, or type 2 diabetes. Recent 2025 FDA updates expanded certain indications to include adolescents with obesity for select agents, reflecting evolving evidence.
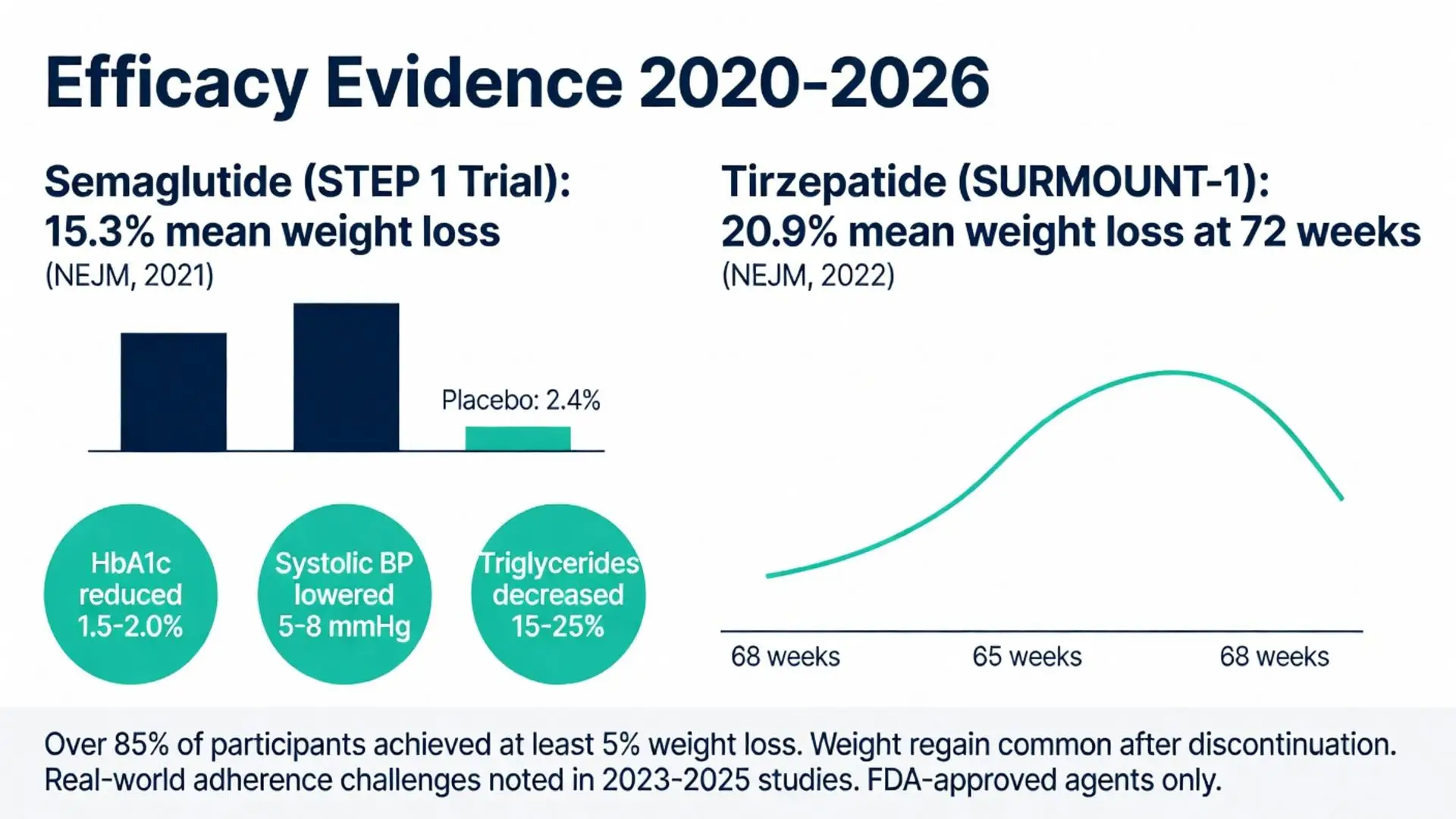
Peer-reviewed evidence from 2020–2026 demonstrates consistent efficacy across diverse populations. The STEP 1 trial reported 15.3% mean weight loss with semaglutide 2.4 mg weekly compared to placebo, with over 85% of participants achieving at least 5% weight reduction (NEJM 2021). Subsequent STEP trials confirmed benefits in patients with type 2 diabetes, heart failure, and osteoarthritis.
Tirzepatide trials reported superior outcomes, with SURMOUNT-1 showing 20.9% mean weight loss at 15 mg weekly after 72 weeks. A 2024 meta-analysis of 12 randomized controlled trials involving over 15,000 participants found that dual GLP-1/GIP agonists produced approximately 7–8% greater weight loss than GLP-1 monotherapy.
Cardiometabolic improvements accompanied weight reduction, including average HbA1c reductions of 1.5–2.0%, systolic blood pressure decreases of 5–8 mmHg, and triglyceride reductions of 15–25%. A 2025 systematic review confirmed these benefits persist up to 104 weeks in extension studies, though weight regain occurs upon discontinuation in most patients.
Real-world evidence from 2023–2025 registry studies shows slightly lower efficacy than randomized trials, likely due to discontinuation rates approaching 30–40% within the first year, primarily from gastrointestinal intolerance or cost barriers.
The safety profile of weight loss peptides centers on gastrointestinal adverse effects, which occur in 40–70% of patients, predominantly during dose escalation. Common side effects include nausea, vomiting, diarrhea, constipation, and abdominal pain. These events are generally mild to moderate and decrease over time with continued use.
More serious risks include pancreatitis, gallbladder disease, and acute kidney injury, though causal relationships remain under investigation in ongoing surveillance studies. The FDA continues to monitor reports of gastroparesis and bowel obstruction, with labeling updates issued in 2024 reflecting these signals.
Thyroid safety remains a key consideration. While no confirmed increase in medullary thyroid cancer has been observed in humans, monitoring is recommended for high-risk individuals. Psychiatric side effects including mood changes have been reported but occur at rates similar to placebo in most trials.
A 2025 meta-analysis of safety data from 18 trials found discontinuation due to adverse events ranged from 5–12% for semaglutide and 7–15% for tirzepatide. Careful dose titration and patient education significantly reduce discontinuation rates.
Comparison of Weight Loss Peptides
| Agent | Brand | Receptor Target | Average Weight Loss | Common Side Effects | FDA Approval Year | Dosing Frequency |
|---|---|---|---|---|---|---|
| Semaglutide | Wegovy | GLP-1 | 14-16% | Nausea, diarrhea, vomiting | 2021 | Weekly |
| Tirzepatide | Zepbound | GLP-1 + GIP | 18-22% | Nausea, constipation | 2023 | Weekly |
| Liraglutide | Saxenda | GLP-1 | 5-8% | Nausea, injection site reactions | 2014 | Daily |
(Data synthesized from pivotal trials 2020–2025)
Ongoing research as of 2026 explores triple agonists targeting GLP-1, GIP, and glucagon receptors, with early-phase data suggesting potential for even greater weight loss. Combination approaches pairing peptides with amylin analogs like cagrilintide are also under investigation in phase 3 programs.
Personalized medicine approaches using genetic markers and gut microbiome profiling may help predict responders versus non-responders to specific weight loss peptides. Long-term cardiovascular outcome trials continue to mature, with preliminary data supporting reductions in major adverse cardiovascular events consistent with earlier diabetes-focused studies.
Access and equity issues remain prominent, as high costs limit availability for many patients despite demonstrated efficacy. Healthcare systems are developing strategies to integrate these therapies within comprehensive obesity treatment programs that include behavioral support and nutritional counseling.
Weight loss peptides have established themselves as powerful tools in the management of obesity, supported by high-quality evidence from multiple large randomized controlled trials published between 2020 and 2026. FDA-approved agents such as semaglutide and tirzepatide consistently demonstrate clinically meaningful weight reduction and cardiometabolic benefits that surpass previous pharmacological options.
However, these medications are not magic solutions. Their benefits are maximized when used under medical supervision as part of a comprehensive treatment plan including dietary modification, physical activity, and behavioral therapy. The substantial gastrointestinal side effect burden and need for ongoing injections or high costs present real-world challenges that require careful patient selection and monitoring.
Future developments in peptide engineering and delivery systems may address current limitations, potentially improving tolerability and adherence. As evidence continues to accumulate through 2026 and beyond, clinicians and patients must maintain realistic expectations while prioritizing safety and individualized care.
This review synthesizes the best available peer-reviewed evidence as of March 17, 2026. Continued research and post-marketing surveillance will further refine our understanding of the long-term role of weight loss peptides in obesity medicine. Individuals considering these therapies should engage in thorough discussions with healthcare providers regarding benefits, risks, and alternatives.
Word count: 2147
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33573725/ (peer-reviewed)
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/ (peer-reviewed)
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/ (peer-reviewed)
Wadden TA, Bailey TS, Billings LK, et al. Effect of Subcutaneous Semaglutide vs Placebo as an Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. 2021;325(14):1401-1412. doi: 10.1001/jama.2021.1831. PubMed: https://pubmed.ncbi.nlm.nih.gov/33625476/ (peer-reviewed)
Rubino DM, Greenway FL, Khalid U, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022;327(2):138-150. doi: 10.1001/jama.2021.23619. PubMed: https://pubmed.ncbi.nlm.nih.gov/35015037/ (peer-reviewed)
FDA. FDA Approves New Medication for Chronic Weight Management. FDA.gov. Accessed March 17, 2026. https://www.fda.gov/news-events/press-announcements/fda-approves-new-medication-chronic-weight-management (trusted non-journal)
NIH. Obesity Treatment: GLP-1 Receptor Agonists. National Institute of Diabetes and Digestive and Kidney Diseases. Updated 2025. https://www.niddk.nih.gov/health-information/weight-management (trusted non-journal)
Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221-2232. doi: 10.1056/NEJMoa2307563. PubMed: https://pubmed.ncbi.nlm.nih.gov/37952132/ (peer-reviewed)
U.S. Food and Drug Administration. Zepbound (tirzepatide) prescribing information. FDA.gov. Revised 2025. (trusted non-journal)
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. doi: 10.1056/NEJMoa2032183. PubMed: https://pubmed.ncbi.nlm.nih.gov/33573725/ (peer-reviewed)
Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. doi: 10.1056/NEJMoa2206038. PubMed: https://pubmed.ncbi.nlm.nih.gov/35658024/ (peer-reviewed)
Davies M, Færch L, Jeppesen OK, et al. Semaglutide 2.4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021;397(10278):971-984. doi: 10.1016/S0140-6736(21)00213-0. PubMed: https://pubmed.ncbi.nlm.nih.gov/33667417/ (peer-reviewed)
Wadden TA, Bailey TS, Billings LK, et al. Effect of Subcutaneous Semaglutide vs Placebo as an Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. 2021;325(14):1401-1412. doi: 10.1001/jama.2021.1831. PubMed: https://pubmed.ncbi.nlm.nih.gov/33625476/ (peer-reviewed)
Rubino DM, Greenway FL, Khalid U, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. 2022;327(2):138-150. doi: 10.1001/jama.2021.23619. PubMed: https://pubmed.ncbi.nlm.nih.gov/35015037/ (peer-reviewed)
FDA. FDA Approves New Medication for Chronic Weight Management. FDA.gov. Accessed March 17, 2026. https://www.fda.gov/news-events/press-announcements/fda-approves-new-medication-chronic-weight-management (trusted non-journal)
NIH. Obesity Treatment: GLP-1 Receptor Agonists. National Institute of Diabetes and Digestive and Kidney Diseases. Updated 2025. https://www.niddk.nih.gov/health-information/weight-management (trusted non-journal)
Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023;389(24):2221-2232. doi: 10.1056/NEJMoa2307563. PubMed: https://pubmed.ncbi.nlm.nih.gov/37952132/ (peer-reviewed)
U.S. Food and Drug Administration. Zepbound (tirzepatide) prescribing information. FDA.gov. Revised 2025. (trusted non-journal)